 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
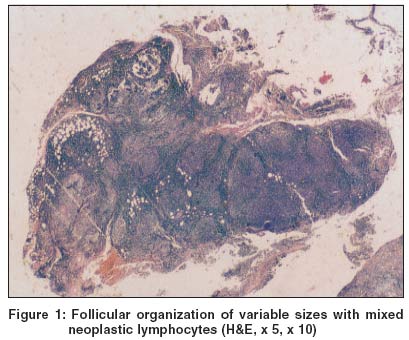
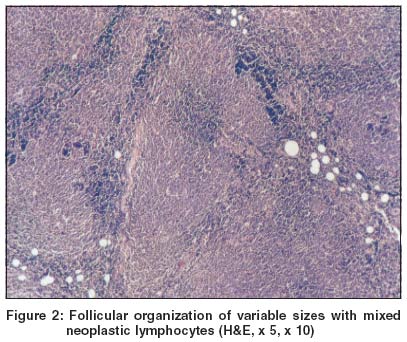
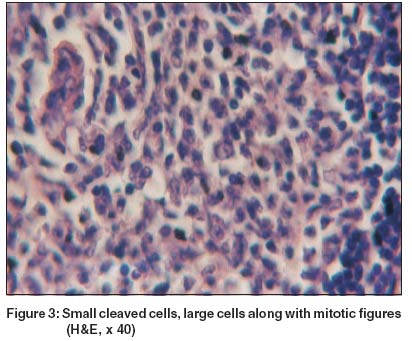
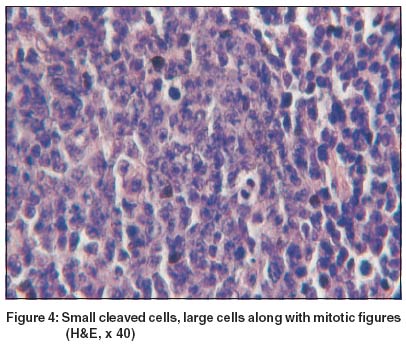
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 172-174 Case Report Primary extranodal non-Hodgkin's lymphoma of the oral cavity Ramani Pratibha , Ahmed Shaheen , Janaki VR Department of Dermatology, Madras Medical College and Hospital, Chennai Code Number: dv04055 ABSTRACT Non-Hodgkin's lymphoma (NHL) belongs to a group of lymphoid neoplasms that is diverse in manner of presentation, response to therapy and prognosis. Usually the oral manifestations of NHL are secondary to a more widespread involvement throughout the body. Though primary intraoral lesions in NHL are uncommon, it is important to be aware of them, since intraoral manifestations are the presenting symptom in these patients. A 55 year old woman presented with a swelling in the maxillary right alveolus and buccal vestibule. There were no palpable lymph nodes. A CT scan revealed a mass on the labial aspect of the right maxilla with no involvement of the maxillary sinus. Incisional biopsy of the lesion showed a dense lymphocytic infiltrate with formation of variably sized lymphoid follicles. The infiltrate showed a mixed neoplastic lymphocyte composition which was suggestive of follicular mixed type of malignant B cell primary extranodal lymphoma. The patient was treated with chemotherapy followed by radiation.INTRODUCTION Oropharyngeal lymphomas are uncommon but most frequently arise in the Waldeyer's ring, which, after the gastrointestinal tract, is the second most common site for extranodal lymphomas.[1] There has been much controversy over the problem of whether malignant lymphomas are multicentric in origin or unicentric. There is general agreement that involvement of lymph nodes is common with oral lymphomas.[2] However our patient did not have any lymph node involvement. CASE REPORT A 55-year-old woman presented with a growth in the upper right alveolus with nasal obstruction for the past 4 months. She had undergone total extraction 3 years back. She did not give any contributory medical and family history. She did not chew tobacco or betel nut. On examination a non-tender, firm swelling involving the right maxillary alveolus extending to the buccal vestibule in the region between teeth number 13 and 17 (right canine to right second molar) was evident. There were no palpable lymph nodes. Investigations revealed normal complete hemogram, blood sugar, and liver and kidney function tests. The patient's ELISA for HIV and VDRL were negative. Scrapings taken from the involved region to rule out fungal granulomas did not show any fungi. A CT scan revealed a mass on the labial aspect of the right maxilla with no involvement of the maxillary sinus. Differential diagnoses of squamous cell carcinoma, deep fungal infections and benign tumors were considered. Histopathology of an incisional biopsy of the lesion showed follicular organization of variable sizes with a mixed neoplastic lymphocyte composition [Figure - 1] consisting of small-cleaved cells having scanty cytoplasm and irregularly cleaved nuclear contour (centrocyte like) [Figure - 2] admixed with large cells containing vesicular nuclei (centroblast like) [Figure - 3] along with mitotic figures [Figure - 4]. These features were consistent with the follicular mixed type of malignant B cell lymphoma. The patient was subjected to chemotherapy followed by radiation and is on regular follow up. DISCUSSION Non-Hodgkin's lymphoma has a varied manner of presentation, response to therapy and prognosis. It rarely manifests as a primary malignancy in the head and neck region (>1%)[3] and may give an important clue for undiagnosed HIV infection, which accounts for 2% of oral neoplasms in patients with AIDS.[4] It more commonly affects the middle aged and the elderly with a slight male preponderance. The gingival and palate regions are commonly affected, while involvement of the alveolus and buccal vestibule, as seen in our patient, is rare. Secondary organ involvement along with the primary in the oral cavity is generally observed,[5] but this was not observed in our patient. The vast majority of lymphomas of the oropharyngeal region are of the B cell rather than the T cell type. The genetic profile for extranodal follicular (mixed type) lymphoma is as follows: Characteristic CD20+, CD3- The differential diagnosis includes benign reactive hyperplasia and other types of lymphomas.[6] Generally a combination of chemotherapy (with cyclophosphamide, doxorubicin, vincristine, prednisone) field radiation is recommended for treatment.[7] Monoclonal antibodies directed against antigens or within the lymphoma and injection of interferon have also been used. The prognosis of the disease is usually relapse free as initial response to treatment is good but the disease has a prolonged course interrupted by therapeutic remissions, and cure is rare with a maximum of 5-year survival rate in 30% of cases after therapy.[8] The disease may occasionally progress into a diffuse pattern with cutaneous nodules and plaques, undergo blast transformation or rarely turn into leukemia. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04055f4.jpg] [dv04055f3.jpg] [dv04055f2.jpg] [dv04055f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}