 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
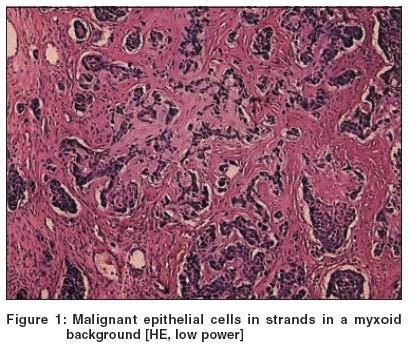
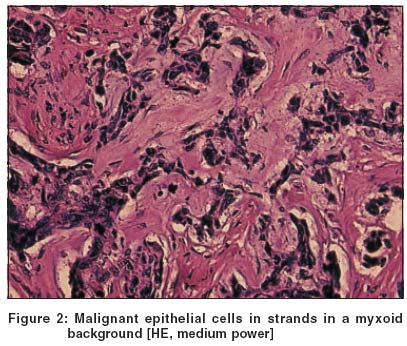
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 175-176 Case Report Malignant chondroid syringoma Shashikala P, Chandrashekhar HR, Sharma Shalini , Suresh KK Department of Pathology, JJM Medical College, Davangere Code Number: dv04056 ABSTRACT An adult female presented with a painful recurrent swelling on the posterior aspect of the scalp of six months' duration, which was clinically diagnosed as fibroma. An excision biopsy showed anaplastic epithelial cells arranged in irregular cords and trabeculae, mitosis, malignant chondroid areas, desmoplasia and perineural invasion, suggesting malignancy. Wide excision of the tumor was the only treatment given since there was no metastasis.INTRODUCTION The diagnosis of adnexal neoplasms presents difficulties related to the large variety of different tumors and their variant forms, and the frequency of differentiation along two or more adnexal lines in the same tumor. Chondroid syringoma is a benign appendageal tumor with eccrine differentiation.[1] The malignant variant of chondroid syringoma is rare. In most cases of malignant chondroid syringoma, anaplastic changes are present from the beginning. Rarely, a chondroid syringoma of many years' duration suddenly undergoes malignant changes with widespread metastasis.[1] CASE REPORT A 32-year-old female was referred to the hospital with the history of a swelling on the posterior aspect of the scalp. The lesion was present since seven years. It had been excised earlier but had recurred; unfortunately, the excised mass had not been sent for histopathology. The lesion had become painful and was increasing rapidly in size for the last six months. Examination revealed an unrelated mass 5 x 4 cm in size with an irregularly nodular surface and firm to hard consistency.The nodule was excised and sent for histopathology. On gross examination, the cut section was diffusely grey white and nodular. Microscopy revealed an intradermal non-encapsulated tumor composed of anaplastic epithelial cells arranged in cords, tubules and trabeculae. [Figure - 1], [Figure - 2] Occasional mitotic figures were seen (0-1/HPF). Malignant chondroid areas and desmoplasia were seen along with perineural and lymphatic invasion. No regional lymph node metastasis or distant metastasis were identified at the time of presentation. DISCUSSION Malignant chondroid syringoma may occur de novo or rarely develop in a chondroid syringoma. In contrast to the benign counterpart, which is common in the head and neck region, the malignant variety occurs predominantly on the trunk and extremities.[2] In our patients, a middle aged woman, the tumor was on the scalp and recurred after previous excision. The female preponderance of this tumor is reported in many studies.[2],[3],[4] Mitosis, nuclear atypia, pleomorphism, lymphatic invasion and local recurrence have been recognized as helpful signs for the diagnosis of malignancy[1],[2],[3],[5] and these features were present in our case. Chondroid syringoma may be confused clinically with epidermal cyst, pilar cyst, calcifying epithelioma or a solitary trichoepithelioma,[6] which is probably the reason for the tumor not being sent for histopathology after excision earlier. Recurrence of the lesion alerts the clinician to the possibility of malignancy.[3],[6] This highlights the need for microscopic diagnosis of all tumors that are excised irrespective of the clinical diagnosis. Treatment consists of complete excision of the tumor. Though local radiotherapy is often unsuccessful, skeletal metastasis has been shown to respond to radiotherapy.[3] Combination chemotherapy in patients with metastasis is not reported to be beneficial.[3] Adequate surgical excision with wide disease free margins is the only hope for disease control.[3] In the present case wide excision of tumor was done the patient was lost to follow up. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04056f2.jpg] [dv04056f1.jpg] |
| |||||||||

{kind=link}
{kind=link}