 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
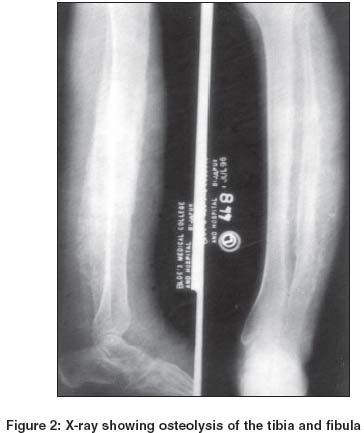
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 177-179 Case Report Vanishing bone disease Inamadar Arun C, Palit Aparna , Korishetti SI Departments of Dermatology, Venereology and Leprology, BLDEA's SBMP Medical College, Hospital & Research Centre, Bijapur, Karnataka Code Number: dv04057 ABSTRACT A young lady presented with progressive hypertrophy and lateral curvature of the left leg of long duration. The overlying skin showed remarkable vascular prominence. The limb involvement was asymptomatic except minor restriction of movements. Radiologically, there was diffuse osteolysis of the tibia and fibula suggestive of vanishing bone disease. This rare condition bears a clinical resemblance to other disorders with vascular malformations and limb hypertrophy. The differential diagnosis of vanishing bone disease, from the dermatologists' point of view has been discussed.INTRODUCTION Vanishing bone disease is characterized by progressive osteolysis of the involved bones. The presenting features are hypertrophy of the involved part, overlying cutaneous vascular malformations and pathological fracture resulting from minor trauma.[1] When the extremities are involved, gross clinical similarities with other conditions like Klippel-Trenauney syndrome, Parkes-Weber syndrome, Proteus syndrome and Maffuci's syndrome may cause diagnostic confusion.[2] Diffuse osteolysis to the extent of total radiological disappearance of the underlying bone helps in distinguishing this condition. The condition is also described as disappearing or phantom bone disease and Gorham-Stout disease. CASE REPORT A 24-year-old lady presented with progressive swelling and lateral bowing of her left leg since childhood. The swelling was painless but recently she had developed restriction of movement of the limb with difficulty in walking. She did not have any systemic complaints. There was no history of any major illness in the past. No other family member was affected with a similar disorder. On examination, the left leg was curved laterally [Figure - 1] and there was a diffuse swelling of the limb, confined strictly below the knee, extending distally to the dorsum of the foot [Figure - 1]. There was a bluish, compressible, tortuous vascular prominence overlying the swollen area, along with hyperpigmentation around the ankle. The temperature of the involved area was normal. No palpable thrill or bruit was present. The Brodie-Trendelenberg test was negative. There was no macrodactyly. The patient was normotensive. A clinical diagnosis of Gorham-Stout disease was made. Routine haematological and biochemical parameters were within normal limits. X-rays of the left leg, AP and lateral views, showed diffuse osteolysis of the tibia and fibula with widening of the medullary cavity and thinning of the cortex, surrounded by a soft tissue swelling [Figure - 2], suggestive of vanishing bone disease. The patient was counseled about the course and prognosis of the disease. DISCUSSION Gorham-Stout disease is a sporadic disorder of unknown etiology. It was first described by L.W. Gorham (1954) in a patient with massive osteolysis and subsequent resorption of the clavicle.[3] The disorder starts in childhood, but in more than one third of the cases, the age at presentation is above 35 years.[4] The shoulder and pelvic girdles are the sites of predilection.[4] Sometimes involvement of the long bones of the extremities is observed, as in the present case. These patients present with limb hypertrophy with overlying cutaneous venous and/or lymphatic malformation, progressive weakness and limitation of movement of the unilateral limb. After several months or years, the limb becomes flail and useless. Pain is not a usual feature and the condition often remains undiagnosed until the patient presents with pain associated with pathological fractures.[5] Crippling deformities may sometimes develop.[4] The characteristic radiological feature is increasing translucency of the involved bone without any sclerosis and progressive resorption of the bony structure.[5] Involvement of the contiguous bones can occur irrespective of intervening joints.[4] Histopathologically, the osseous tissue is replaced by thin walled, sinusoidal blood vessels without reactive bone formation.[4] It is a rare disorder and reports in the literature are sparse. In 1955, Gorham and Stout reported a series of 24 patients.[6] In a recent report by Gerharz et al,[1] a middle aged man with involvement of both long and short bones of the lower limb with progressive pain has been described. Though rare, this entity constitutes an important differential diagnosis of other conditions with co-existent vascular malformations and limb hypertrophy.[7] Klippel-Trenauney syndrome is the triad of port-wine stain, venous and lymphatic malformations and overgrowth of all tissues, particularly the bone of an affected limb. Lower limb involvement is common and increased limb length is characteristic. Radiologically, cortical thickening of the hypertrophic bone is observed. Osteoporosis is a late feature. In Parkes-Weber syndrome, limb hypertrophy is associated with a port-wine stain and multiple arteriovenous fistulae. The affected limb is large, warm with pulsation and bruit. The arm is more commonly affected than the leg. In Proteus syndrome, limb hypertrophy and port-wine stain are associated with a variety of distinctive abnormalities like macrodactyly and lipoma like subcutaneous hamartomas. The predominant sites of involvement in Maffuci's syndrome are the hands and feet. Cutaneous venous malformations are associated with multiple radiolucent enchondromas. None of these conditions develop diffuse osteolysis as observed in Gorham-Stout disease. The course of Gorham-Stout disease is unpredictable. Usually the condition is slowly progressive. Sometimes the course may be aggressive and complicated by Kasabach-Meritt syndrome.[8] Rarely, spontaneous arrest of the progression can occur. No effective treatment is available. Radiotherapy may be considered in the pres-ence of bone pain and incipient pathological fracture.[9] REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04057f2.jpg] [dv04057f1.jpg] |
| |||||||||

{kind=link}
{kind=link}