 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
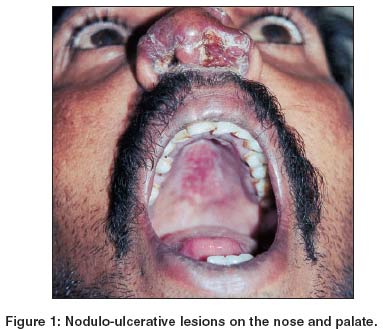
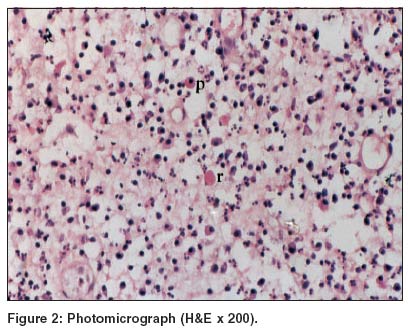
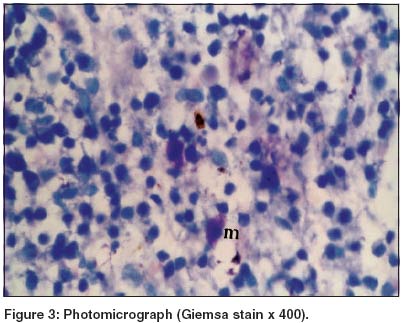
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 3, May-June, 2004, pp. 197-198 Quiz Nodulo-ulcerative lesions over the nose Inamadar Arun C, Palit Aparna , Kulkarni NH, Guggarigoudar SP, Yelikar BR Department of Dermatology, Venereology and Leprosy, BLDEA's SBMP Medical College, Hospital and Research Centre, Bijapur Code Number: dv04067 A 41-year-old agricultural worker presented with asymptomatic nodulo-ulcerative lesions on the nose and adjacent areas, hoarseness of voice and difficulty in swallowing for the past 2 months. He had been suffering from progressive nasal stuffiness for the past 4 years. He was otherwise healthy and had no systemic complaints. On examination, there were indurated, ulcerative, plaques involving the dorsum of the nose, columella and adjacent parts of the philtrum. A hard nodular mass with variegated surface was present at the vestibule of the nose on the left side, obstructing the whole anterior nares [Figure - 1]. An indurated painless ulcer about 2 cm x 2.5 cm in size was observed on the hard palate. The lesions on the nose were mildly tender without any discharge. Gram stained smear and culture from the lesions on the nose did not reveal any specific organism. A biopsy was taken from the nodular lesion [Figure - 2], [Figure - 3]. A Leishman stained imprint smear from the biopsied tissue did not reveal any organism. WHAT IS THE DIAGNOSIS? Answer:H&E stained histopathological examination [Figure - 2] showed diffuse plasma cell infiltration (p) in the dermis. Eosinophilic Russell bodies (r) were seen. Mikulicz cells (m) were seen in Giemsa stained histopathological preparation [Figure - 3]. Intracellular organisms were not demonstrable. On the basis of the clinical and histopathological findings, the patient was diagnosed as a case of rhinoscleroma in the granulomatous stage. He was treated with ciprofloxacin (500 mg BID) and rifampicin (450 mg OD), and has been kept under follow-up. DISCUSSION Rhinoscleroma is a chronic granulomatous infection caused by a Gram negative, capsulated, bacillus Klebsiella rhinoscleromatis.[1] Sporadic cases occur throughout the world with endemicity in some countries.[2] Overcrowded housing conditions and direct or indirect contact with the nasal exudate of an infected person facilitates transmission. The disease onset is insidious, with a mild nasal discharge and crusting (catarrhal stage). Gradually nodulo-ulcerative lesions develop involving the nose, upper lip, palate and adjacent regions of the upper respiratory tract (granulomatous stage). The lesion is dusky red, stony hard, insensitive to touch and minimally tender. Intranasal rubbery, polypoidal lesions are common. In the advanced stage, there is destruction of the nasal cartilages with resultant deformity (Hebra nose). This is followed by a marked tendency to fibrosis and subsequent obstruction (sclerotic stage). In the granulomatous stage it can be mistaken for mucocutaneous leishmaniasis, rhinosporidiosis, lupus vulgaris, sarcoidosis, Wegener's granulomatosis or a carcinoma.[1],[2] Prolonged administration of antibiotics like tetracyclines, co-trimoxazole, ciprofloxacin and rifampicin, is the mainstay of therapy. The infection is persistent and relapse is common even with complete treatment. Laryngeal obstruction is a rare complication that may be fatal.[3] The histopathological picture in the granulomatous stage is highly characteristic.[1] Dense plasma cell infiltration with Mikulicz cells and Russell bodies are seen. A Mikulicz cell is a large, round, vacuolated histiocyte with a pale, reticulate, poorly defined cytoplasm, eccentric nucleus and intracellular organisms, better visualized in Gram, Giemsa, PAS or Warthin-Starry stained preparations. A Russell body or colloid body is an elliptical, eosinophilic structure in the cytoplasm of plasma cells. Rhinoscleroma has a close histopathological resemblance to donovanosis, leishmaniasis and other chronic granulomatous infections.[4] Plasma cell infiltration and Russell bodies may also be seen in chronic infections like treponematosis, cutaneous amebiasis, leishmaniasis and tuberculosis. However, the clinical features help in differentiation from other granulomatous conditions. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04067f3.jpg] [dv04067f1.jpg] [dv04067f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}