 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
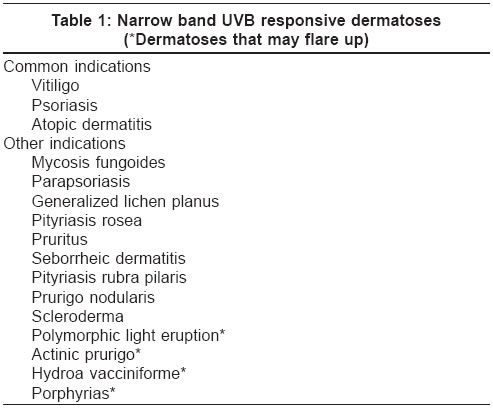
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 205-209 Review Article Narrow band UVB phototherapy in dermatology Dogra Sunil, Kanwar AmrinderJit Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education & Research, Chandigarh Code Number: dv04070 HISTORICAL ASPECTS The first report of the use of ′phototherapy′in the treatment of skin disorders dates from 1400 BC from India when patients with vitiligo were given certain plant extracts (whose active ingredients included psoralens) and then exposed to the sun.[1] The real interest in the use of ultraviolet (UV) irradiation in the treatment of various skin diseases started in the 19th century when Niels Finsen received the Nobel Prize (1903) for his therapeutic results with UV irradiation in lupus vulgaris, the only dermatologist ever to be awarded one.[2] This marked the start of modern phototherapy. It was used in thermal stations for the treatment of tuberculosis, in the treatment of leg ulcers in wartime, and various other skin diseases.[3] It was a very long journey from the use of plant extracts and sun exposure to treat vitiligo to the use of oral psoralens and total body UVA-irradiation cabins (PUVA) to treat various skin diseases. In a landmark development, in 1974 Parrish et al reported the useful role of high intensity UVA tubes in combination with oral psoralens in the treatment of psoriasis leading to what is now known as PUVA therapy.[4] The history of UVB phototherapy is not as old as the history of photochemotherapy. Wiskemann introduced irradiation cabin with broad band UVB tubes in 1978 for the treatment of psoriasis and uremic pruritus.[5] However, broad band UVB phototherapy was less efficient for treating psoriasis than PUVA and so never achieved popularity. The breakthrough came after 1988 when narrow-band UVB (NB-UVB) phototherapy was introduced for the treatment of psoriasis by van Weelden et al and Green et al.[6],[7] THERAPEUTIC SPECTRUM A potential advance in UVB-based phototherapy has been the introduction of fluorescent bulbs (Phillips model TL-01) that deliver UVB in the range of 310 to 315 nm, with a peak at 312 nm. It has a relatively narrow spectrum of emission which when compared with the older broad band UVB source has a reduction in erythemogenic wavelengths in the 290-305 nm range and 5-6 fold increased emission of the longer UVB wavelengths, thereby resulting in a higher phototherapy index for psoriasis.MECHANISM OF ACTION In the skin, NB-UVB radiation is absorbed by DNA and urocanic acid and alters antigen presenting cell activity. NB-UVB is about 5-10 fold less potent than broad band UVB for erythema induction, hyperplasia, edema, sunburn cell formation and Langerhans cell depletion from the skin. It has a relatively more suppressive effect than broad band UVB on systemic immune responses as judged by natural killer cell activity, lymphoproliferation and cytokine responses.[8] The mechanism of action of NB-UVB phototherapy has not been completely understood. In psoriatics, NB-UVB phototherapy lowers peripheral natural killer cell activity, lymphocyte proliferation and immune regulatory cytokine production by both Th1 (IL-2, IFN-g) and Th2 (IL-10) T-cell populations.[8],[9] Similar to PUVA therapy, NB-UVB may exert its effects in vitiligo in a two-step process. Both steps may occur simultaneously, the first being the stabilization of the depigmenting process and the second, the stimulation of residual follicular melanocytes.[10],[11] The well-documented immunomodulating effects of UV radiation can explain the stabilization of the local and systemic abnormal immune responses.[12] It is also likely that NB-UVB, similar to PUVA therapy, stimulates the dopa-negative, amelanotic melanocytes in the outer hair "root sheaths, which are activated to proliferate," produce melanin and migrate outward to adjacent depigmented skin resulting in perifollicular repigmentation.[11] The ability of NB-UVB radiation to systemically suppress the major components of cell mediated immune function is thus likely to be linked to its beneficial effect in several inflammatory skin diseases including psoriasis. PHOTOTHERAPY UNIT NB-UVB phototherapy cabins contain fluorescent TL-01 (100 W) tubes as the source of irradiation. The cost of a chamber and lamps show considerable variations between countries and distributors. NB-UVB cabins available commercially either incorporate TL-01 alone or in combination with UVA tubes. Combination chambers take longer to administer a treatment dose. Thus, although they provide flexibility, they may represent an unsatisfactory compromise for a busy phototherapy unit. Recently, shorter tubes of NB-UVB have also become available in small area treatment equipments (hand and foot unit, NB-UVB comb) for the therapy of localized body areas.DOSING SCHEDULE NB-UVB schedules can be tailored according to patient skin type and local experience. There are two regimens that are most commonly used; the first involves determination of the individual′s minimum erythema dose (MED) by means of a separate bank of TL-01 tubes. Often 70% of the MED value is used for the first treatment; thereafter therapy is given three times or more in a week with 40, 20 or 10% increments depending on local experience and skin type tolerance. Another approach, as commonly practiced in India, involves a standard starting dose (280 mJ/cm2), with stepwise increase (usually 20%) depending upon the patient′s erythema response. In the photodermatoses, the approach is more cautious with only 10% incremental regimen on sun-exposed sites.[9] In case of mild erythema, the irradiation dose is held constant for subsequent treatments or until resolution of symptoms. The goal of therapy is to achieve persistent asymptomatic erythema. In case of painful erythema "with or without edema/blistering, further treatment is" withheld till the symptoms subside. After resolution of overdose symptoms, the dose administered is 50% of the last dose and subsequent increments should be by 10%.INDICATIONS 1. Vitiligo In 1997, Westerhof and Nieuweboers-Krobotova[13] first reported the use of NB-UVB phototherapy for the treatment of vitiligo. In their comparative study, 67% of patients undergoing NB-UVB phototherapy showed repigmentation compared with 46% of patients receiving topical PUVA after 4 months of therapy. In a recently published study, NB-UVB was reported to be effective and safe in childhood vitiligo.[14] In this open trial, 51 children with generalized vitiligo were treated twice weekly with NB-UVB radiation therapy for a maximum period of 1 year, resulting in more than 75% overall repigmentation in 53% of patients and stabilization of disease in 80%. Scherschun et al retrospectively analyzed their experience of treating vitiligo with NB-UVB administered as monotherapy 3 times a week.[15] Five of their seven patients achieved more than 75% repigmentation with a mean of 19 treatments, whereas the remaining two patients had 50% and 40% repigmentation after 46 and 48 treatments respectively. In a recent meta-analysis of non-surgical therapies in generalized vitiligo by Njoo et al,[19] higher success rates were observed with NB-UVB (63%) than with oral PUVA (51%). As in the western population, NB-UVB phototherapy produces a cosmetically good color match in Indian patients.[18] Its distinct advantages over PUVA include the lack of psoralen related side effects and precautions, cosmetically better color match, and its safety in children. However, the relative stability of NB-UVB induced repigmentation over PUVA, its maximum safe duration and cumulative dose allowed still remain to be determined. 2. Psoriasis Although treatment with NB-UVB is reported to be highly effective in clearing psoriasis patients, whether this therapy represents a modest advance or a real breakthrough is not clear. If NB-UVB is to replace PUVA therapy in the treatment of more severe psoriasis, it must not only achieve a comparable clearance rate in psoriasis, but it must also maintain remission at a comparable frequency of treatment. At present, small studies do provide some hope in this respect.[26]
3. Atopic dermatitis 4. Other dermatoses COMBINATION THERAPY In psoriasis, NB-UVB has been used in combination with topical therapies like tar, dithranol, calcipotriol and tazarotene. There are some reports suggesting faster clearance, but the benefit of their combination with NB-UVB over NB-UVB used alone in the treatment of psoriasis is still debatable.[33],[34] However, it should be remembered that for most patients an attractive feature of NB-UVB monotherapy is the absence of topical therapy. There is hardly any published information on the role of combination therapy in vitiligo. Broad band UVB has also been used in combination with psoralen (PUVB),[35] but its comparative efficacy and safety over NB-UVB and PUVA remain to be determined.EVIDENCE BASED CURRENT USE In Europe, NB-UVB phototherapy is being increasingly used for the treatment of various skin diseases including psoriasis. Irradiation with this source has been found to be superior to conventional broad band UVB in psoriasis, producing longer remissions, a lower incidence of burning and possibly a lower risk of UV carcinogenesis.[25],[36] In an important attempt to develop evidence-based guidelines for the treatment of vitiligo, NB-UVB therapy was recommended as the most effective and safest therapy for generalized vitiligo.[37] The general advantages of NB-UVB therapy over PUVA include safe use in children and pregnant women, no need for post-treatment eye protection, no drug induced nausea and no drug costs.LONG TERM USE AND ADVERSE EFFECTS As with other forms of UV exposure, in addition to the expected immediate sunburn effects, chronic NB-UVB exposure is likely to increase photoaging and the risk of carcinogenesis.[8] Presently there is insufficient human data available to provide recommendations regarding the safe maximum NB-UVB dose. However, according to a dose response model it has been calculated that the long-term risk for carcinogenesis with its use may be less than that of PUVA therapy.[38] Clinical experience with NB-UVB is limited and currently there is no established safe limit for its maximum safe duration of use in vitiligo. Njoo et al recommend that responsive patients can be given this treatment for a maximum of 24 months.[37] After the first course of one year, they recommend a resting period of three months to minimize the annual cumulative dose of UVB. In children, the maximum duration allowed is 12 months. Subsequently, if required, only limited areas should be exposed. If no response is observed after six months, further therapy should be discouraged. Further, the risk of cutaneous malignancies in vitiligo can be reduced by skin saving principles, i.e. covering the parts that have repigmented satisfactorily and shielding the genitals.REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04070t1.jpg] |
| |||||||||

{kind=link}