 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
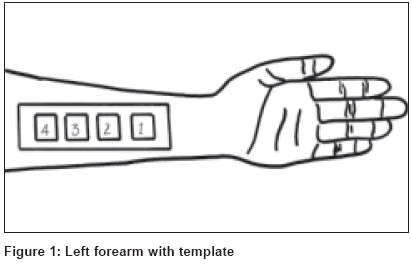
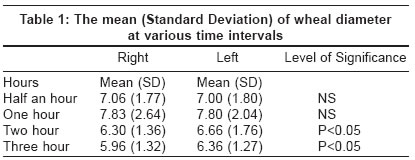
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 214-216 Studies Half an hour versus three hour contact of topical steroid (clobetasol propionate) Rai Reena, Uppal Monica, Sharma NarashimaK, Srinivas CR, Mathew Anil Dept. of Dermatology, PSG Institute of Medical Sciences & Research, Coimbatore Code Number: dv04072 ABSTRACT BACKGROUND: Steroids when left on the skin for longer duration may contribute to the side effects without any additional clinical benefit. The relationship between the duration of topical steroid contact with the skin and its effectiveness has not been established. The ability of the topical steroids to inhibit the size of histamine induced wheal was used to assess their relative efficacy. AIM: To determine whether half an hour contact and three hour contact of a topical steroid, clobetasol propionate, is equally effective in inhibiting the size of the histamine induced wheal. METHODS: On 30 volunteers, 4 squares were marked on flexor aspect of both forearms using a template. One fingertip unit of clobetasol propionate 0.05% was applied on all the areas. Half an hour later all areas of left forearm and last square of right forearm were wiped. Prick testing was done with histamine and size of wheal recorded after 15 minutes. Similarly steroid was wiped from the 1st, 2nd, 3rd square after 1 hr, 2 hr and 3 hrs on right forearm and the corresponding areas prick tested on both forearms. RESULTS: There was statistically significant wheal suppression at the end of 2 hrs and 3hrs as compared to half an hour. CONCLUSION: We conclude that half an hour application of clobetasol propionate is ineffective and that it is effective only after two hours of contact and hence short contact of half an hour will be less effective than relatively prolonged contact of 2 hours. Keywords: Topical corticosteroid, histamine induced wheal, clobetasol propionate INTRODUCTION Topical steroids are widely used for various dermatoses. Studies have shown that once daily application of topical steroid is as effective as twice daily.[1] Few studies compare the efficacy of steroids with different duration of contact of steroids with the skin. Topical steroids inhibit histamine and increase peripheral resistance.[2] The ability of the topical steroids to inhibit the size of histamine induced wheal was used to assess their relative efficacy. The relationship between the duration of topical steroid contact with the skin and its effectiveness has not been established. We hypothesize that, steroids when left on the skin for longer duration may contribute to the side effects without any additional clinical benefit. This study was conducted to determine whether half an hour contact and three hour contact of topical steroid is equally effective in inhibiting the size of the histamine induced wheal.METHODS Thirty volunteers who had not used systemic or topical corticosteroids, antihistamines for at-least 8 weeks and not on any other drugs for at-least 7 days were studied. Pregnant and lactating females, individuals with history of atopy, history of any systemic disease or skin infection were excluded from the study. A template was made using plastic transparent sheet with 4 apertures (3 x 3 cm) cut 2 cm apart. The template was placed on both forearms and with a marker pen each aperture was outlined. The squares on both forearms were numbered 1, 2, 3, and 4 [Figure - 1]. One fingertip unit of clobetasol propionate 0.05% (©Tenovate) was applied at each site. The steroid ointment on all squares of left forearm and the first square of right forearm was wiped after 30 minutes with a dry gauze piece. Prick testing was done on the first square on both forearms by standard method. A drop of 0.1% w/v histamine solution was placed on the test site. Skin was pricked through the histamine solution with a lancet. The tip was kept parallel to the skin surface and skin was lifted by tenting the lancet by 45 to 60 degrees. After one minute the test sites were dabbed with filter paper to remove the excess histamine solution. The size of the wheal was recorded in millimeters after 15 min. The mean size of the wheal was calculated by measuring the maximum diameter and the orthogonal diameter of the wheal with a transparent scale. Similarly 2nd, 3rd and 4th squares on the right forearm were wiped at the end of 1 hr, 2 hrs and 3 hrs. The corresponding areas on both forearms were prick tested with histamine and the results recorded. RESULTS The mean diameter of the wheal after ½ hr, 1 hr, 2 hr, 3 hr is shown in [Table - 1]. The results were analyzed by paired t-test.DISCUSSION Topical corticosteroids are frequently used. Few pharmacodynamic data is available on topical steroids, despite their extensive use in the treatment of skin diseases since 1952.[3] The ability of topical corticosteroids to suppress the size of wheals induced with histamine on skin has been used to assess their relative efficacy.[4] Although it is a non-clinical assay, it possesses close similarity to processes involved in the development of clinical dermatoses.[4] The mechanism of action of topical corticosteroids are quite complex and affect many systems. Topical glucocorticoids have both immediate and delayed effects. The immediate effect may be due to direct steroid incorporation into membranes, thereby preventing release of lysosomal contents and phospholipid precursors for synthesis of prostaglandins and platelet-activating factor.[5] The delayed effects appear to be due to glucocorticoid alteration of DNA transcription via a second messenger system initiated by steroid. The corticosteroid diffuses into the target cell and binds to the steroid receptor.[6] This steroid receptor complex enters the nucleus and binds to specific locations on DNA, modulating transcription of genes coding for proteins that are responsible for the biological effects of the steroids.[7] We hypothesize that the additional application of topical corticosteroid after saturation is unlikely to be of therapeutic benefit and it may contribute to the side effects of steroids. The goal of the treatment is to achieve maximum desired effect and minimum undesired effect. Topical steroids inhibit histamine release and reduce sensitivity of vascular smooth muscle to histamine and increase peripheral resistance.[2] The histamine bioassay of topical corticosteroids has many advantages over the other known assay techniques. It is a simple, reliable, and reproducible procedure. The end point of the assay is very easy to observe. Skin colour does not interfere with the interpretation of the results.[4] Hence this method was used to determine the effect of duration of contact of topical steroid. We conclude that half an hour application is ineffective and the preparation of clobetasol used in this study (©Tenovate) is effective only after two hours of contact and hence short contact of half an hour will be less effective than relatively prolonged contact of 2 hours. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04072t1.jpg] [dv04072f1.jpg] |
| |||||||||

{kind=link}
{kind=link}