 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
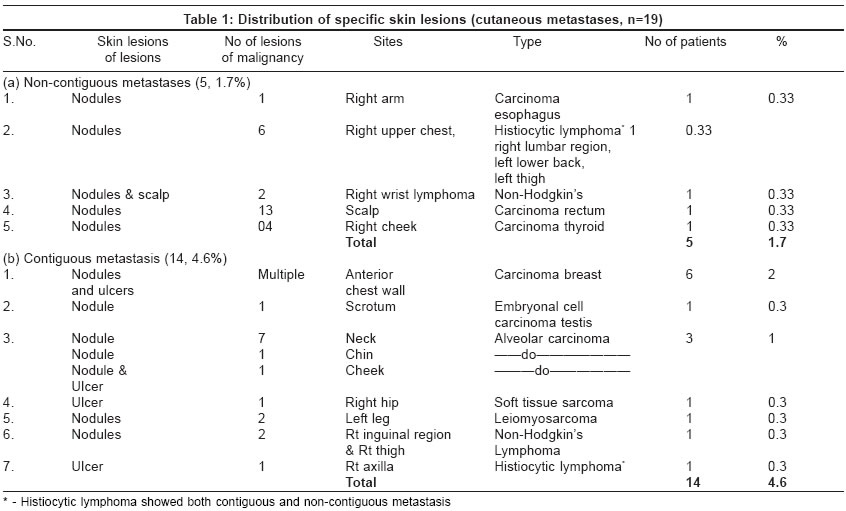
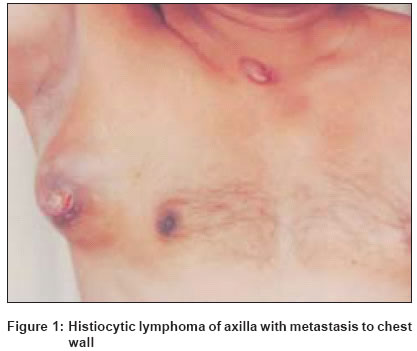
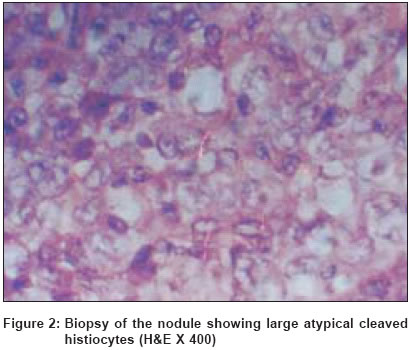
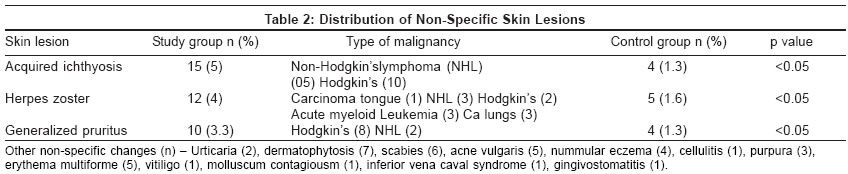
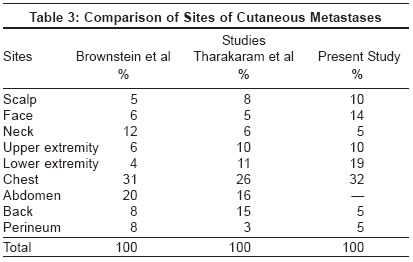
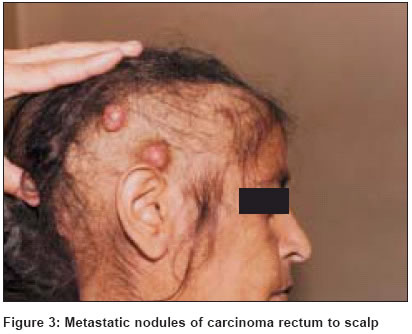
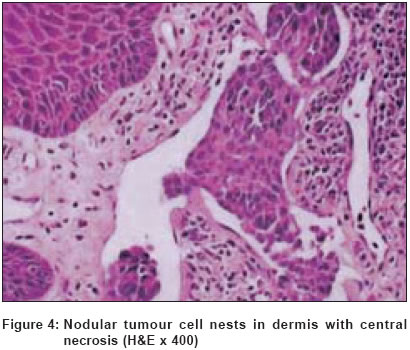
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 221-225 Studies Skin changes in internal malignancy Rajagopal Ravi, Arora PN, Ramasastry CV, Kar PK Dept of Dermatology, 5 Air Force Hospital, C/o 99 APO Code Number: dv04074 ABSTRACT BACKGROUND: Internal malignancies are accompanied by various skin changes which may be specific infiltrates or non-specific changes. This study is aimed at determining the frequency of such changes in malignant disease treatment center attendees in India. METHODS: A study of 300 confirmed cases of internal malignancy at a malignant disease treatment center was undertaken to evaluate these skin changes. Specific infiltrates were confirmed by histopathology. Statistical methods were employed to calculate significance in non-specific lesions by comparing with 300 controls not suffering from internal malignancy. RESULTS: Skin changes were present in 82 (27.3%). Cutaneous metastases were found in 19 (6.3%); non-contiguous in 5 (1.6%); contiguous in 14 (4.3%). Non-specific skin lesions numbered 74 (11.6%) in 52 patients. Statistically significant non-specific skin changes were acquired ichthyosis, herpes zoster and generalized pruritus. CONCLUSION: Metastases usually occurred late in internal malignancy (17, 5.6%) except in a case each of histiocytic lymphoma and non-Hodgkin's lymphoma (2, 0.7%) where the lesions preceded malignancy by 3 months and 1 month respectively. Contiguous nodules were a marker of relapse after surgery in 3 (1%). Keywords: Cutaneous metastases, malignant neoplasms INTRODUCTION The human integument mirrors many internal disorders. Internal malignancies may give rise to a number of cutaneous disorders through their immunological, metabolic and metastatic consequences. These changes can be divided into specific malignant infiltrates and non-specific lesions. Specific infiltrates that show characteristic malignant cells on histopathological examination can occur due to contiguous or non-contiguous spread. Non-specific lesions can be classified into infections, non-infective conditions and changes due to chemotherapy.METHODS Three hundred cases of internal malignancies of varying duration involving different body organs, from two malignant disease treatment facilities, were recorded over a period of one year for skin changes. Only those confirmed to be having a malignant disease were included. Those cases that proved to be negative for malignancy after investigation were excluded. History was recorded for the duration of the malignancy as well as the duration of skin change, detailed cutaneous and systemic examination was done, clinical photographs were taken, skin biopsy was performed where required, scrapings done for fungal infections and follow-up was done for progress of the lesion. Special stains were used for histopathology of the specific infiltrates. All cutaneous metastatic lesions were verified by histopathology. Another 300 cases admitted for non-dermatological and non-malignant diseases were taken up as controls for the comparison of the frequency of non-specific lesions. RESULTS Of the 300 cases studies 156 (52%) were males and 144 (48%) females. One hundred and two patients (34%), were above the age of 51 years, 72 (24%) in the fourth decade, 61 (20.3%) in the age group 31-40 years, 49 (16%) in the age group 21-30 years, 7 (2.3%) in the age group 11-20, and 9 (3%) below the age of 10 years. The commonest malignancies in males were lymphomas in 26(8.6%), brain tumors in 25 (8.3%) followed by carcinoma of the lungs in 16 (5.3%). The commonest malignancy encountered in females was carcinoma of the breast in 30 (10%), followed by carcinoma of the cervix in 15 (5%), malignancies of the upper respiratory tract in 12 (4%), kidney and bladder tumors in 11 (3.6%), and carcinoma of the ovary in 10 (3.3%). Skin changes were present in 82 patients (27.3%) out of the 300 studied. Specific skin infiltrates (cutaneous metastases) numbered 19 (6.3%), non-specific skin lesions were 74 (24.6%) in 52 patients as more than one manifestation was present in one patient, and drug reactions in 10 (3.3%). One case (0.3%) of genetic disorder with an increased predisposition to develop malignancy was noted in a case of neurofibromatosis that later developed retroperitoneal malignant fibrous histiocytoma. Cutaneous metastasis was contiguous in 14 (4.6%) cases and non-contiguous in 5 (1.6%) cases. Details of the sites and diagnoses of these cases are mentioned in [Table - 1]. The case of histiocytic lymphoma had both contiguous and non-contiguous metastasis. There were 2 (0.6%) cases of metastatic nodules manifesting as the presenting sign of internal malignancy. The first was in a case of histiocytic lymphoma where the nodules appeared two months prior to the axillary swelling [Figure - 1]-[Figure - 2]. The other was in a case of non-Hodgkin′s lymphoma with the skin lesion on the hand appearing a month prior to the swelling over the neck. All the other lesions appeared 3-5 years after the initial malignancy. Six (2%) cases of cutaneous metastasis died within varying periods of metastasis. Two of the 6 cases of carcinoma breast survived for a period of 24 months following the appearance of metastatic lesions. The others responded to aggressive surgery and radiotherapy. The case of carcinoma rectum succumbed within 6 months of onset of skin metastasis. One case each of carcinoma alveolus, non-Hodgkin′s lymphoma and carcinoma thyroid had survival times of 12 months, 15 months and 18 months respectively. Skin metastases indicated relapse after surgery in 3 (1%) cases. These were noted in a case of carcinoma alveolus, a case of non-Hodgkin′s lymphoma and a case of leiomyosarcoma leg. Non-specific skin lesions numbered 74 (24.6%) in 52 patients as more than one change was present in one patient. The most common and significant non-specific skin lesions as compared to the controls are summarized in [Table - 2]. Drug eruptions constituted a total of 10 (3.3%) cases. Flagellate pigmentation and lichenoid drug eruption were noticed in one case each (0.3%) due to bleomycin and cisplatin respectively. Acneiform drug eruption due to steroids was seen in two cases (0.6%) and nail pigmentation in one (0.3%). Generalized hyperpigmentation due to hydroxyurea was seen in 5 (1.6%) cases. DISCUSSION The single most basic biologic process that characterizes a malignant tumor is the ability to produce secondary deposits (metastases) at distant sites. The skin is an infrequent site for metastasis and was listed in one study[1] as only the eighteenth most common site. Cutaneous metastases can arise at any age. However, in keeping with the increased incidence of malignant disease in later life, most cutaneous metastases occurred during or after the fifth decade.[2] The incidence of cutaneous metastases was maximum in the 51 years and above age group (55%). Skin metastases were reported in different studies[3],[4] in 3-4% of cases. In the present study the incidence is 6.3% [Table - 1]. The higher incidence is probably due to the fact that skin infiltrates by leukemias and lymphomas were included as well as direct extension and ulceration by malignancy. Cutaneous metastatic lesions are usually multiple and their number may range from one to hundred.[5] In the present study also, 4 of 5 cases with non-contiguous metastases and 9 of 14 cases with contiguous metastases had multiple lesions [Table - 1]. The most common internal malignancies to give rise to cutaneous metastases are carcinomas of the lung and colon in males and carcinoma of the colon and ovary in females. Overall, melanomas are the commonest followed by carcinoma breast, carcinomas of oral cavity, lungs, colon and ovary.[6] However, in this study, carcinoma breast was the commonest, followed by lymphomas, oral cavity, and GI tract. The difference in the findings may be due to the more common occurrence of lymphomas and the exclusion of melanomas in this study. The anterior chest wall was reported[6],[7] as the most common site for cutaneous metastatic lesions and it held good for this study as well wherein 32% of the lesions were in the chest wall [Table - 3]. However, the face and the lower extremities were the next most common sites for metastasis. The abdomen formed the second most common site in other studies.[6],[7] However, in this study, there were no metastatic lesions on the abdomen. In the other studies,[6],[7] malignant melanoma was also included for the purpose of cutaneous metastasis, which was excluded in this study, as the study was restricted to internal malignancy. This could account for the difference in observations. The scalp formed an unusual site for cutaneous metastasis in a case of carcinoma rectum [Figure - 3]- [Figure - 4]. Carcinoma esophagus was an uncommon cause for cutaneous metastasis, responsible only in 15 (2%) of 724 cases and 9 of 588 (1.5%) cases of cutaneous metastasis in two different studies[6],[8] and the metastases were multiple. In the present case there was one case (0.3%) of esophageal carcinoma and the metastasis was solitary. Cutaneous metastasis as the first sign of internal malignancy has been reported in carcinoma lung, hepatocarcinoma, renal adenocarcinoma, adenocarcinoma esophagus as well as malignant histiocytic lymphomas.[9] In this study, too, two cases of lymphomas, one of the histiocytic type and one of the non-Hodgkin′s type showed cutaneous metastases as the first sign of underlying malignancy. Metastases to the skin usually signify a hopeless outcome and the patients survived for an average of 3 months in one study.[4] In the present series, 6 (2%) cases of cutaneous metastases succumbed to their illness. Carcinoma rectum had the shortest survival time of 6 months, while one case each of carcinoma alveolus, non-Hodgkin′s lymphoma and carcinoma thyroid had survival times of 12 months, 15 months and 18 months respectively. Two cases of carcinoma breast had survival periods of 24 months, while the other cases were surviving at 5 years follow-up. The survival times compared well with those of earlier studies.[10] Some studies also report longer survival for periods ranging from 1 to 4 to even 10 ½ years.[5],[11] There was one case of neurofibromatosis in a 17-year-old girl who developed high-grade malignant fibrous histiocytoma in the retroperitoneum. However, this malignancy has been reported in neurofibromatosis only once before in the literature.[12] Three non-specific skin changes were found with increased predisposition in patients with malignant diseases as compared to controls and those were acquired ichthyosis, generalized pruritus, and herpes zoster. All cases of acquired ichthyosis had lymphomas. Both acquired ichthyosis and generalized pruritus were more common in Hodgkin′s lymphomas than in non-Hodgkin′s lymphoma as reported by other workers[13] [Table - 2]. Drug-induced changes constituted an interesting finding of flagellate pigmentation by bleomycin given for testicular tumor. Flagellate pigmentation that is normally caused by busulfan was found to be caused by bleomycin in this study. Generalized hyperpigmentation was found to be caused by hydroxyurea as is known and vincristine caused bluish nail pigmentation. Cutaneous metastases are relatively uncommon but they are important to recognize. They may precede malignancy as in a case of histiocytic lymphoma in the present study. Contiguous metastases are most common in carcinoma of breast and oral cavity and often herald the recurrence of malignancy after surgery. The trunk and the scalp are favored sites for distant metastases. The mortality rate is usually high with cutaneous metastases though early recognition offers some chance of survival, especially in those that present with cutaneous metastases. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04074f4.jpg] [dv04074t3.jpg] [dv04074t1.jpg] [dv04074f3.jpg] [dv04074f2.jpg] [dv04074t2.jpg] [dv04074f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}