 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
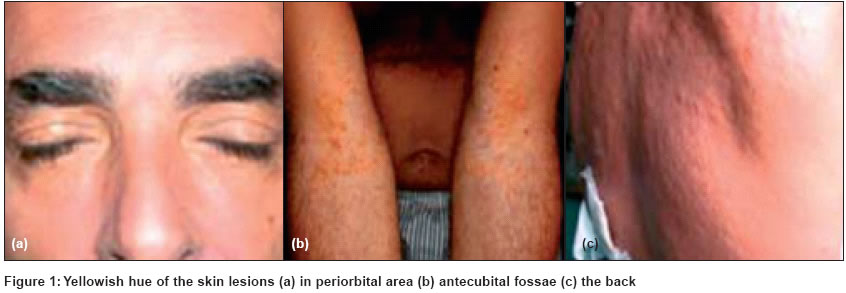
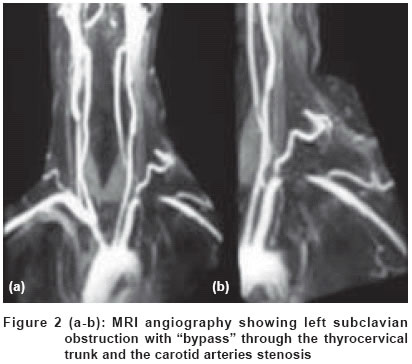
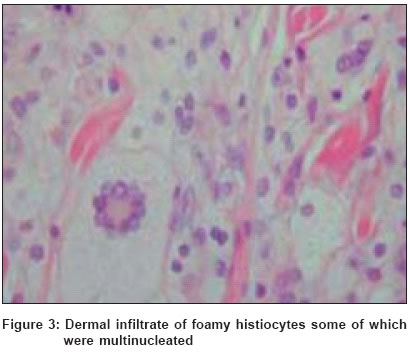
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 230-233 Case Report Diffuse plane normolipemic xanthomatosis associated with Takayasu's disease and hyperhomocysteinemia: A case report Fichera Giampiero, Anastasio Eduardo, Capasso Fabrizio, D'Avino Maria, Margarita Annamaria, Caruso Domenico 12th Unit of Internal Medicine, A.O.R.N. A. Cardarelli Hospital, Naples Code Number: dv04076 ABSTRACT We describe a case of diffuse plane normolipemic xanthomatosis (DPNX) associated with Takayasu's disease and hyperhomocysteinemia. This report of an association of Takayasu's disease with hyperhomocysteinemia and DPNX is the only such report in literature. This report corroborates the study by Marcoval et al on 8 patients in 1988 where they highlighted that in every case of DPNX a possible concomitant condition should be always suspected and found out. Keywords: Diffuse plane normolipemic xanthomatosis, Takayasu, hyperhomocysteinemia INTRODUCTION Diffuse plane normolipemic xanthomatosis (DPNX) is a rare condition whose significance and nosologic position is still uncertain.[1],[2],[3] Although there are only a handful of reports of DPNX, many seem to suggest only an isolated skin pathology. In fact, we came across a report that almost always a monoclonal component is associated with the cutaneous accumulation of lipids. However, some cases of "essential" DPNX have been described that are not associated with any pathologies.[2],[3] We describe a case of DPNX for the first time associated with Takayasu′s disease and hyperhomocysteinemia. CASE REPORT A 52-year-old white male, ex-smoker came to us with symptoms of syncope. He had been affected by arterial hypertension (AH) for several years. The yellowish hue of the skin had begun about 7-8 years ago and had gradually extended to the periorbital areas, back, neck and the main body folds. It was not associated with other disorders like fever, pruritus, etc. He had noticed a decrease in strength of his radial pulse, and most recently discomfort of his left biceps after extended periods of use. There was no history of arthralgias, myalgias, weight loss, asthenia, headache, jaw claudication, fever, diarrhea, abdominal pain, viral infections or neurological disorders. Physical examination revealed that the blood pressure in the right arm measured 170/100 mmHg and in the left arm, 120/70 mmHg (difference between arms > 30 mmHg). The left radial pulse was barely detectable. There was no acral hypoperfusion or cardiac murmurs, but there were bruits on the carotid arteries, subclavian arteries, femoral arteries, renal arteries and abdominal aorta. Yellowish patches-plaques were just visible on both sides of the periocular area and on the neck. They were also evident in the folds of the elbows and knees, back, right buttock and right side of the groin. The entire back was almost completely covered by the skin lesions and its surface was fairly irregular due to the presence of micro- and macro-papules [Figure - 1a-c]. Laboratory tests results were as follows: ESR 90; C-reactive protein 8.9 (normal value < 5 mg/dl); presence of monoclonal component (MC) IgG-ê only in the sera (4.94 g/l;. n.v. 2-4.4 g/l); mild leukocytosis (WBC 18,000 mm3, with 73% of neutrophils); no anemia; complement within normal limits; ANA (antinuclear antibodies), Anti-Sm antibodies, anti-ENA (extranuclear antigens), ANCA absent; LDH, CPK, fibrinogen within normal limits; IgG, IgA, and IgM within normal limits; latex test and RA test within normal limits; circulating immunocomplexes (CIC) absent. There was no alteration in the lymphocytic typing. ApoA1 (1.24 g/l; n.v. 1.1-2.05), ApoB (1.14 g/l; n.v. 0.6-1.3), triglycerides (145 mg/dl; n.v. <160 mg/dl) and HDL (68 mg/dl; n.v.>60 mg/dl), LDL (76 mg/dl; n.v. <130 mg/dl), cholesterol (180 mg/dl; n.v. < 200); no abnormality in C, S protein amount; anti-phospholipid antibodies; anti-cardiolipin IgG and IgM, and anti-thrombin III were within normal limits; no factor V Leiden; â2 microglobulins within normal limits; blood calcium and phosphorous within normal limits; T3, T4 and TSH within normal range; anti-thyroglobulin antibodies and anti-thyroperoxidase (TPO) antibodies absent; high levels of homocysteine (Hcy): 42 µmol/l (n.v.<13 µmol/l); von Willebrand factor within normal range whereas the endothelins levels were high; negative stool specimen for parasitic infestation; anti-HIV, HCV, EBV, HSV, CMV and rickettsia antibodies absent; V.D.R.L negative. The electrocardiogram, echocardiogram, Holter monitoring, chest X-ray, electroencephalogram, and brain CT and MRI were all normal. Skeletal survey revealed no osteolysis or osteoporosis. Fundoscopy and ultrasonography of the upper and lower abdomen were also normal. The renal arteries resistance index was within the norm (0.64 for the right hilus and 0.61 for interlobular arteries; 0.67 for the left hilus and 0.62 for the interlobular arteries). Ultrasound Doppler of the aortic arch branches revealed strong hyperplasia of the medium tunica at the left common carotid artery level extending to the inner and outer homolateral carotid artery, which caused patency reduction of 54%, 45% and 78% respectively. This hyperplasia was also evident in the right side at the common carotid artery and the homolateral outer carotid artery and caused patency reduction of 55%. The hyperplasia also affected the left subclavian artery and caused patency reduction of 90%. Brain and abdominal MRI angiography revealed about 60% stenosis of the right common carotid artery′s fork extending to the homolateral outer carotid artery origin. A lesser degree of stenosis of the left common carotid artery was also present. Further there was left subclavian obstruction just after the thyrocervical origin point which appeared hypertrophic. The abdominal aorta presented on the axial planes a thickening of the anterior wall just above the level of the renal artery [Figure - 2a-b]. The skin biopsy revealed diffuse dermal infiltration by foamy histiocytes some of which were multinucleated [Figure - 3]. No amyloid fibrils were observed and Congo red reaction was negative. Bone marrow biopsy revealed just a marginal increase of plasma cells (5-6%). DISCUSSION According to the facts that we registered, we diagnosed DPNX associated with Takayasu′s disease type 1[11] and hyperhomocysteinemia. For Takayasu′s disease we observed the ACR diagnostic criteria modified by Ishikawa[12] and by Sharma[13] which are as follows:
Our patient had 5 positive ACR criteria (A-E) and 1 major criterion and 4 minor criteria positive according to the Ishikawa/Sharma criteria (F + G, H, M, Q). We began therapy with prednisolone 1 mg/kg per day for six months, cyclophosphamide 2 mg/kg per day for 1 year, and folic acid 10 mg/day for 3 months. Although an "essential" DPNX has been described,[2],[3] generally it is associated with a monoclonal component (either benign or as epiphenomenon of severe hemopathies like lymphomas or myelomas). On rare occasions other associations have been observed: erythema nodosum and relapsing polychondritis,[4] arthritis,[5] serositis and vasculitis,[6] temporal arteritis and retinal vasculitis,[7] cutaneous vasculitis,[8] amyloidosis,[9] mycosis fungoides[10]. It is hypothesized that immunoglobulins produced by these patients have anti-beta lipoproteic activity creating circulating immune complexes and consuming complement.[14] These immune complexes, whose clearance could also be reduced, accumulate in dermal macrophages. The association with vasculitis would lead one to think that these immune complex deposits start an inflammatory process in the vessel walls. It is possible that the lipid metabolism disorder activated by the monoclonal component, and with an anomalous or no longer balanced lipoprotein (the apolipoprotein B has atherogenic properties), may also influence "normolipemic" atheromatosis which adds to the vascular damage. Finally, we can state that the additional presence of hyperhomocysteinemia in the patient we observed could play a role in the vascular damage. We believe that our case is unique. Our findings are basically in line with the study by Marcoval et al[15] on 8 patients in 1988 where the authors highlight that a concomitant condition should always be suspected in every case of DPNX. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04076f3.jpg] [dv04076f2.jpg] [dv04076f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}