 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
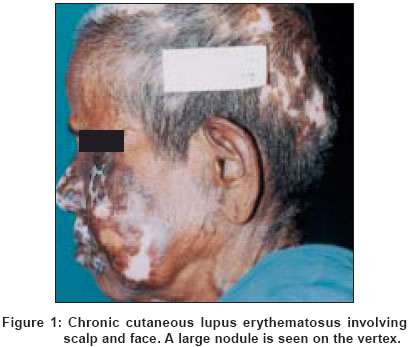
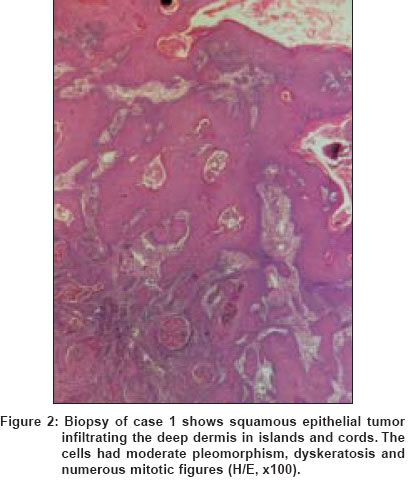
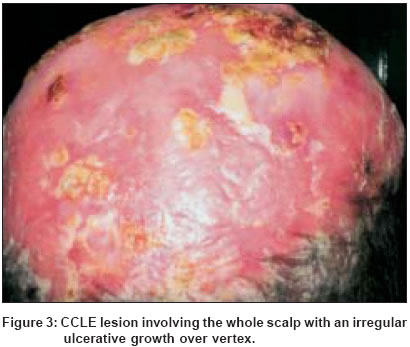
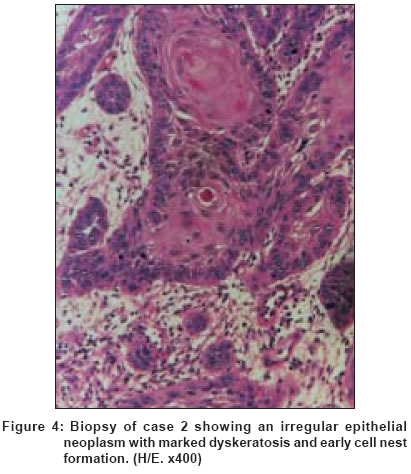
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 236-238 Case Report Squamous cell carcinoma of the scalp arising from chronic cutaneous lupus erythematosus: Report of two Indian patients Kar BikashRanjan, Nair Vinod, Ebenezer Gigi, Job CK Departments of Dermatology, Schieffelin Leprosy Research & Training Centre, Karigiri, Vellore Code Number: dv04078 ABSTRACT Squamous cell carcinoma (SCC) usually arises in skin damaged by actinic rays. Exposure to chemicals like coal tar, soot, arsenic and a variety of oils and distillation products is also implicated in its pathogenesis. It occasionally occurs in scars following inflammatory or degenerative processes. It is an end stage complication of a wide array of inflammatory skin conditions. SCC complicating chronic cutaneous lupus erythematosus (CCLE) in Indian patients is rarely reported. Here we report two such Indian patients with long standing CCLE in whom the diagnosis of CCLE and SCC was confirmed by histopathology. Keywords: Squamous cell carcinoma, cutaneous lupus erythematosus INTRODUCTION Squamous cell carcinoma is one of the serious and potentially life-threatening complications of CCLE. Though rare, this complication is often reported in western literature.[1] The paucity of reports of this complication in Indian literature warrants its mention.CASE 1 A 75-year-old lady from south India presented with a complaint of multiple, depressed, depigmented lesions on the scalp and face for 14 years. She also noticed a swelling on the scalp since one year. On examination, there were multiple atrophic plaques with follicular plugging, mild scaling and a hyperpigmented margin varying in size from 0.5 x 0.5 cm to 4 x 3 cm. There was a dome shaped, cauliflower like growth-measuring 3 x 2 cm overlying the depigmented plaque on the vertex of her scalp [Figure - 1]. The tumor was friable and bled on touch. No regional nodes were palpable. A clinical diagnosis of discoid lupus erythematosus with moderately differentiated squamous cell carcinoma was made. Routine investigations of blood, urine and stool were noncontributory except that the hemoglobin was 9 g%. The chest X-ray was normal. A biopsy revealed epithelium with basket weave orthokeratosis, mild atrophy and follicular plugging. The basal layer showed hydropic degeneration. The dermis showed a dense inflammatory infiltrate composed of lymphocytes, histiocytes and plasma cells around the blood vessels and skin adnexa. An incisional biopsy from the margin of the tumor revealed hyperplasia of the epithelium with cells infiltrating the deep dermis in islands and cords. The cells showed moderate pleomorphism, dyskeratosis and numerous abnormal mitotic figures. Occasional cell nests were also seen. The dermis also had a lymphohistiocytic infiltrate around the blood vessels [Figure - 2]. A diagnosis of well differentiated squamous cell carcinoma was made. CASE 2 A 64-year-old man reported to the Dermatology Department with complaints of multiple depigmented, scaly lesions on his scalp, face, neck, upper trunk and upper limbs since 20 years. He noticed an irregular growth on the vertex since 6 months, which was expanding slowly with frequent ulceration and bleeding. On examination, the major portion of his scalp was involved by a large depigmented scaly plaque, extending at places to the hairline. He also had multiple atrophic, scaly papulo-plaques with follicular plugging and a hyperpigmented margin, varying in size from 0.5 x 0.5 cm to 4 x 3 cm, distributed over his face, upper limbs and upper portion of his trunk. No evidence of mucosal involvement was present. There was an irregular growth present over the scalp, approximately 5 x 4 cm in size, soft, friable and bleeding on touch [Figure - 3]. The regional nodes were not palpable. A clinical diagnosis of disseminated CCLE with a squamous cell carcinoma was made. A complete hemogram revealed hemoglobin of 10.6 g% and a raised ESR. Other investigations including urine examination and chest X-ray revealed no abnormalities. Antinuclear antibody was negative. Two independent biopsies were taken. A biopsy from the clinically suggestive CCLE lesion over the upper back was consistent with CCLE, while the other, taken from the growth, was consistent with squamous cell carcinoma [Figure - 4]. DISCUSSION SCC and, less commonly, basal cell carcinoma (BCC) are the most feared complications of CCLE. In one study by Millard et al, the incidence was 3.3% among 120 white patients with CCLE.[1] Although carcinoma is considered to occur more commonly in patients who have had radiotherapy for CCLE, 65 out of 100 cases did not have such treatment in their series. Since the substitution of steroids and antimalarials for irradiation in the treatment of CCLE, SCC arising in CCLE is rare. SCC superimposed on a wide array of skin conditions like burn scars,[2] necrobiosis lipoidica diabeticorum,[3] porokeratosis,[4] epidermolysis bullosa,[5] lichen planus[6] and chronic osteomyelitis[7] has also been reported. The scalp is the commonest site involved, as seen in our patients, followed by the lips.[1] Only a few isolated case reports of SCC complicating CCLE in Indian patients are available.[8],[9],[10] The most likely predisposing factors in our patients are old age and a long-standing history of exposure to the sun.REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04078f2.jpg] [dv04078f4.jpg] [dv04078f3.jpg] [dv04078f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}