 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
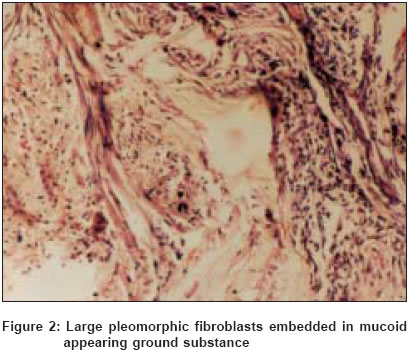
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 239-241 Case Report Nodular fasciitis Cyriac MJ, Celine MI, Kurien George, Puthiode Usha Departments of Dermatology, Medical College, Kottayam, Kerala Code Number: dv04079 ABSTRACT A 24-year-old female presented with a firm, hyperpigmented, and gradually enlarging, tender, solitary dermal nodule of non-traumatic origin over the right suprascapular region. The lesion was extending into the subcutaneous tissue. She was otherwise normal. There was no calcification on X-ray. Biopsy revealed numerous large pleomorphic fibroblasts in a mucoid ground substance diagnostic of nodular fasciitis. No recurrence was noticed after surgical excision. This case is reported because of its rarity in the Indian medical literature. Keywords: Nodular fasciitis, proliferative fasciitis INTRODUCTION Nodular fasciitis (NF) is a benign mesenchymal neoplasm that appears as a firm, solitary nodule with an average diameter of 1 to 5 cm, occasionally tender and located most often on the arm.[1],[2],[3],[4] It may extend into the subcutaneous tissue and muscles. It is seen in otherwise normal healthy individuals with peak occurrence between 20 and 35 years of age.[3] Histopathology reveals the nodule to consist of numerous large, pleomorphic fibroblasts in a highly vascularized stroma containing varying amounts of mucoid ground substance, reticulum and collagen fibers. Scattered erythrocytes along with small lymphocytes may also be present. The component cells have now been shown to be myofibroblasts.[5] We are reporting a case of nodular fasciitis in a woman who presented with a hyperpigmented, hard, dermal nodule extending deep into the subcutaneous tissue over the right suprascapular region. CASE REPORT A 24-year-old woman presented with a gradually enlarging swelling over the right suprascapular region of eighteen months′duration. There was no prior history of trauma. On examination a dermal nodule of 5 cm, hard in consistency and tender on pressure, extending to the subcutaneous fat, was located just above the upper margin of the right scapula. Its surface was hyperpigmented with minimal dimpling at the centre [Figure - 1]. The margins were irregular and mobility was restricted in the horizontal plane. The mucosae, hair and nails were normal. There was no evidence of any systemic involvement. The clinical findings prompted differential diagnoses of calcinosis cutis, dermatofibroma, granular cell myoblastoma and other tumors of fibroblastic origin. An X-ray of the soft tissue did not reveal any evidence of calcification. A biopsy was taken under local anesthesia cutting deep into the lesion. Histopathology revealed numerous large pleomorphic fibroblasts embedded in a mucoid appearing ground substance, features diagnostic of nodular fasciitis. Numerous well formed capillaries were also seen. An infiltrate composed of chronic inflammatory cells was present towards the periphery of the nodule [Figure - 2]. The lesion was surgically excised and no recurrence was noticed on follow up for one year. DISCUSSION Nodular fasciitis was first described by Konwaler and Weiss in 1955[6] and was called pseudosarcomatous fasciitis because of its rapid growth and histologic features.[2] It often begins as a solitary subcutaneous nodule that develops rapidly, reaching an ultimate size of 1-5 cm within a few weeks. The lesion is self-limited, regressing in a few months.[2],[4] The longest known duration is 26 months. Although the forearms and the arms are the most common sites, it may arise from the subcutaneous tissue, muscle or fascia at any location.[3] These tumors are also reported in the orbit and on the oral mucosa.[4] The sex distribution is equal. Symptoms such as numbness, paresthesia or shooting pain are less frequent, but when present indicate compression of a peripheral nerve.[3] The etiology of nodular fasciitis is unknown. The role of trauma in initiating the lesion is doubtful. The myofibroblast is thought to be the cell of origin. Nodular fasciitis is believed to occur as an unusual proliferation of myofibroblasts triggered by local injury or inflammatory processes.[3] Nodular fasciitis occurs as three types according to the plane of tissue involved: subcutaneous, intramuscular and fascial. The lesion is usually attached to the fascia from which it arises and extends into the subcutaneous fat in an irregular fashion. Occasionally it arises from the fibrous septa of the subcutaneous fat and only secondarily extends to the fascia. The nodule consists of numerous whorls of pleomorphic fibroblasts growing haphazardly in the stroma that is often highly vascular and contains varying amounts of mucoid substance, reticulum and collagen fibres.[5] Erythrocytes are present in the capillaries, in slit like spaces as well as free in the tissues. The fibroblasts show a fair number of mitoses which do not appear atypical. In about half the cases small spindle shaped giant cells are found. A scattered chronic inflammatory infiltrate is often present particularly at the periphery of the nodule. Immunohistochemistry has shown that the spindle cells in nodular fasciitis are positive for vimentin, variably positive for actin, and negative for desmin, keratin, or S100 protein.[7] Variants of nodular fasciitis occur deep and are named proliferative fasciitis, cranial fasciitis and proliferative myositis. These variants tend to have clusters of large epithelioid cells with a slightly basophilic cytoplasm and large nuclei.[8] Proliferative fasciitis appears to be related to nodular fasciitis,
but histologically it shows giant cells resembling ganglion cells,
showing an abundant irregularly outlined basophilic cytoplasm with
one or more large vesicular nuclei. The cells are fibroblasts and are
actin negative. The lesion may be occasionally misdiagnosed as rhabdomyosarcoma
or ganglioneuroblastoma.[8] The dermal variant of nodular fasciitis has the typical histology of ordinary nodular fasciitis but may also extend within blood vessels in a manner similar to so-called intravascular fasciitis, a benign variant.[8] The most frequent problem is differentiation between nodular fasciitis, fibrosarcoma, and leiomyosarcoma. The small size, sharp circumscription, myxoid matrix, and scattered erythrocytes and lymphocytes are helpful features for a diagnosis of nodular fasciitis.[8] Nodular fasciitis lacks nuclear atypia, but the appearance of the ganglion like cells in variants of nodular fasciitis can lead to diagnostic confusion with malignant fibrous histiocytoma. Leiomyosarcomas may also be confused with nodular fasciitis, and both can have strong reactivity for actin and numerous mitoses. Leiomyosarcomas are also reactive for desmin and have more cytologic atypia than the cells of nodular fasciitis. Local excision is the treatment of choice of nodular fasciitis and recurrences are rare.[1] The condition has an excellent prognosis. Spontaneous regression has been reported. Rapid resolution of the nodule has been reported to occur with intralesional corticosteroid injection by Graham et al.[3] This is recommended when the lesion cannot be completely excised as when it extends into the muscle. Our patient had a relatively slow evolution. The site reported commonly is the upper arm. In our patient the lesion was located over the upper back. The lesion showed hyperpigmentation which may have been due to hemorrhage occurring into the lesion. The diagnosis was based on the typical histological findings as it is difficult to arrive at a correct diagnosis clinically due to lack of clear cut clinical features. However we would suggest the following points as clinical clues for diagnosis of nodular fasciitis: (a) rapidly growing dermal/subcutaneous nodule not more than
5 cm in size, REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04079f1.jpg] [dv04079f2.jpg] |
| |||||||||

{kind=link}
{kind=link}