 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
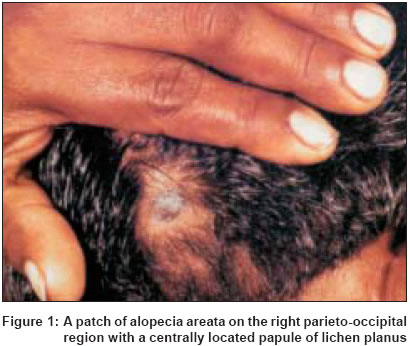
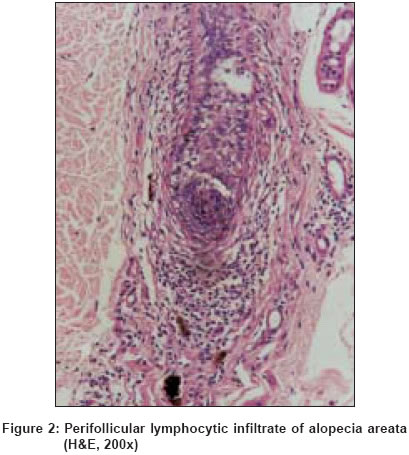
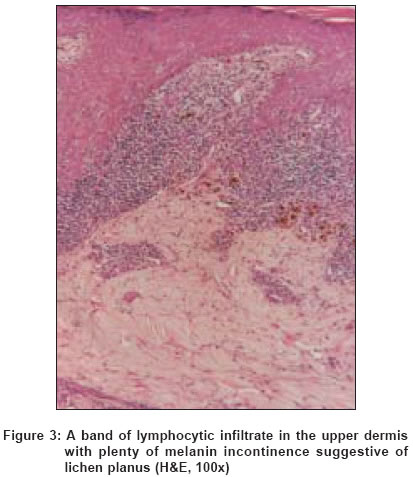
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 242-243 Letter To Editor Colocalisation of alopecia areata and lichen planus Kar BikashRanjan, Ebenezer Gigi, Job CK Departments of Dermatology, Schieffelin Leprosy Research & Training Centre, Karigiri, Vellore Code Number: dv04080 Sir, Frequent associations between alopecia areata and immune-mediated cutaneous disorders have been reported.[1] Being common skin disorders, lichen planus and alopecia areata may rarely coexist. We report a case of co-localization of lichen planus and alopecia areata. A 42-year-old man presented with a single patch of non-scarring hair loss of 4 months′ duration over the right parieto-occipital region. Alopecia areata was diagnosed and he was treated with topical betamethasone dipropionate. With that the lesion became static. He had no other lesion on any hair-bearing area. Three months after the appearance of the initial lesion he developed a solitary violaceous papule in the center of the patch [Figure - 1]. The lesion was pruritic and mildly scaly. No mucosal lesion was present. A biopsy from the patch of alopecia revealed a typical perifollicular "swarm of bees" type lymphocytic infiltrate consistent with a diagnosis of alopecia areata (AA) [Figure - 2]. A biopsy from the central papular lesion showed hyperkeratosis, wedge-shaped hypergranulosis, irregular acanthosis, basal cell liquefaction and a band-like lymphocytic infiltrate and pigment incontinence in the superficial dermis suggestive of a diagnosis of lichen planus (LP) [Figure - 3]. Kanwar et al reported 20-nail dystrophy in a patient of AA due to LP.[2] Brenner et al reported a case of coincidence of five dermatological disorders: vitiligo, AA, onychodystrophy, morphea and LP.[3] Similarly, ulcerative colitis, myasthenia gravis, LP, AA and vitiligo were present in a single patient reported.[4] Patients with AA were found to be at a higher risk for developing LP (RR=2.7; 95% confidence interval, 1.1 to 6.5).[5] However, co-localization is very rare. Dhar et al had reported one child with co-localization of lesions both conditions.[6] The incidence of AA in the Indian population is 0.7%7 whereas it is 0.8% for LP.8 The coexistence of these disorders may be purely coincidental. Gilhar et al found that induction of AA was possible with injection of CD8+ cells cultured with follicular homogenate but not with cultured CD4+ cells.[9] The T lymphocyte is also pivotal in regulating epidermal cell recognition and epithelial destruction in lichen planus. T cells become activated via antigen-presenting cells such as Langerhans cells in conjunction with epidermal keratinocytes and co-stimulatory molecules. Though both CD4+ and CD8+ T cells are found in the lesional skin of LP, progression of disease leads to the preferen-tial accumulation of CD8+ cells.[10] The majority of the lymphocytes in the infiltrate of LP are CD8+ and CD45RO (memory)-positive cells and express the g/d T-cell-receptor. The ensuing immune reaction by CD8+ T lymphocytes against activated keratinocytes results in epidermal cell damage and development of the lichenoid reaction that is the hallmark of lichen planus. Further studies might clarify whether co-localization of lichen planus and alopecia areata is a mere coincidence or represents a common pathogenic mechanism in these two predominantly CD8+ T lymphocyte-mediated disorders. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04080f1.jpg] [dv04080f2.jpg] [dv04080f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}