 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
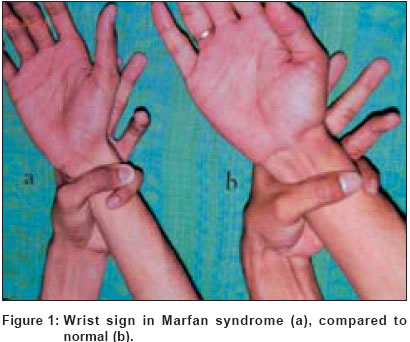
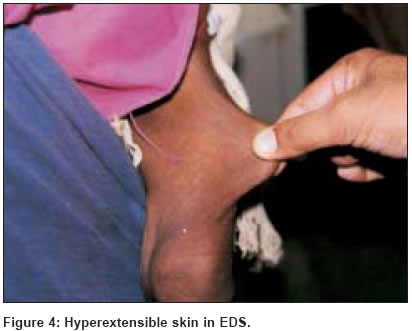
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 4, July-August, 2004, pp. 253-255 Residents' Page Cutaneous signs in heritable disorders of the connective tissue Inamadar ArunC, Palit Aparna Department of Dermatology, Venereology & Leprosy, BLDEA's SBMP Medical College, Hospital & Research Centre, Bijapur Code Number: dv04089 Heritable disorders of the connective tissue are caused by genetic mutations affecting individual components like collagen and elastin or enzymes regulating their metabolism. The important disorders in this group include Marfan syndrome, Ehlers-Danlos syndrome, cutis laxa and pseudoxanthoma elasticum.These disorders present with widespread manifestations involving the skin as well as different systems. Cardiovascular, skeletal and ophthalmic manifestations are frequently seen. Hence, all these disorders are associated with significant disability and life-threatening complications.[1] These patients are seen by dermatologists because the cutaneous manifestations may cause cosmetic handicaps. Often cutaneous features provide the initial clue to the diagnosis. Some of these disorders have overlapping clinical pictures like joint hypermobility and hyperextensibility of the skin and identification of the particular disease becomes difficult. Patients with Marfan syndrome present with unusually tall habitus, long, thin extremities, arachnodactyly and sometimes, joint hypermobility. An abnormally low upper segment (US): lower segment (LS) ratio is characteristic and is indicative of excessive length of the lower extremities.[2] Similarly, armspan (fingertip to fingertip) exceeding the individual′s height indicates increased length of the upper extremities.[2] However, in the presence of moderate to severe kyphoscoliosis, which is a common skeletal deformity in patients with Marfan syndrome, the US: LS ratio and armspan should not be tested.[2] Wrist sign is the overlapping of the thumb and fifth fingers when these encircle the opposite wrist [Figure - 1]. Thumb sign (Steinberg sign)[2] is the extension of the thumb past the ulnar border of the hand, when apposed to the palm [Figure - 2]. These features reflect narrow palm, metacarpal overgrowth and joint hypermobility seen in these patients.[3] Ability to touch the umbilicus with the right hand, crossing the back and approaching from the left side also indicates increased limb length and joint hypermobility. Patients with homocystinuria have a Marfanoid habitus but mild restriction of joint movements is characteristic rather than the hypermobility.[1] Wrist sign and thumb signs are not demonstrable here. In other conditions with marfanoid habitus,[4] like MEN type IIb, congenital contractural arachnodactyly (Beal′s syndrome) and Shprintzen-Goldberg syndrome, these signs may be demonstrable. Patients with Ehlers-Danlos syndrome (EDS) types III and VII present with joint hypermobility and hyperextensible skin. Here the hypermobility is usually limited to the digits, and repeated dislocation of the large joints is characteristic. Arachnodactyly is absent.[1] Beighton sign[2] [Figure - 3] is the passive apposition of the thumb to the flexor aspect of the forearm. It is demonstrable in patients with EDS and indicates joint hypermobility. Beighton sign is part of the Beighton′s criteria for detecting joint hypermobility in adolescents and adults.[2] The skin in patients with EDS is soft, velvety and hyperextensible [Figure - 4]. If pulled out in a fold, it rapidly retracts following release. This feature is responsible for the origin of the name "India-rubber man" in circuses in earlier days. Hyperextensibility of the skin may give rise to gaping "fish-mouth wounds" over bony prominences like the shins, knees, and elbows following minor trauma. Scars following trauma or surgical procedures are thin, atrophic and stretch considerably after healing. Such wide, thin, papyraceous scars over the knees and elbows are called "cigarette paper scars." Two types of soft tissue growths are observed in EDS: molluscoid pseudotumors and spheroids. Molluscoid pseudotumors are bluish-grey, spongy nodules seen over easily traumatized areas like the shin, forearm and tendo-achilles. These are herniations of subcutaneous fat through atrophic dermal scars. Spheroids are buck-shot sized, hard, calcified, subcutaneous nodules resulting from fat necrosis. Gorlin′s sign[2],[4] is the ability to touch the tip of the nose by extension of the tongue [Figure - 5]. It is demonstrable in 50% of patients with EDS and represents hyperextensibility of the tongue. However, 10% of the normal population is also able to perform this action. The upper eyelids can be easily inverted in patients with EDS. Hyperextensibility of skin is also a feature of cutis laxa. In contrast to EDS after stretching, the skin resumes its normal shape only slowly.[2] The inelastic skin gives rise to large pendulous facial folds and prominent nasolabial furrows. In combination with down-slanting palpebral fissures, redundant eyelids, broad, flat nose and large ears, patients assume a characteristic "bloodhound facies." Unlike EDS, joint laxity is not a feature of cutis laxa.[2] Pseudoxanthoma elasticum (PXE) is a unique disorder with predominant cardiovascular and ophthalmologic involvement. Cutaneous signs are subtle and need a high degree of clinical suspicion. Yellowish, flat-topped, discrete and/or confluent papular lesions simulating xanthomas are observed on the sides of the neck, axillae, periumbilical area and perineum. This "plucked chicken skin" or "Moroccan leather" appearance is quite characteristic of PXE.[1],[2] This clinical feature is exaggerated with advancing age with the appearance of redundant skin folds over the involved areas.[1] Umbilicated papules in annular, arciform or serpiginous configuration are a hallmark of elastosis perforans serpiginosa (EPS). In about 40% cases EPS occurs in association with heritable connective tissue disorders like PXE, EDS, Marfan syndrome, osteogenesis imperfecta or acrogeria.[1] EPS begins as small papules that develop a small umbilication covered with a keratotic plug or a crust. The lesions heal spontaneously to leave behind an atrophic scar. The neck, face and proximal extremities are common sites. A recently described[5] cutaneous sign in patients with PXE is "prominent mental (chin) crease." Accentuated creases with horizontal and oblique components extending from the oral commissures down to the sides of jaw are characteristic. Occurrence of this feature in patients with PXE compared to age and sex matched controls bears high sensitivity and specificity for diagnosis.[5] Minor clinical features like these are particularly helpful in a busy outpatient department for quick initial screening of patients with suspected heritable disorders of connective tissue. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04089f4.jpg] [dv04089f3.jpg] [dv04089f1.jpg] [dv04089f2.jpg] [dv04089f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}