 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
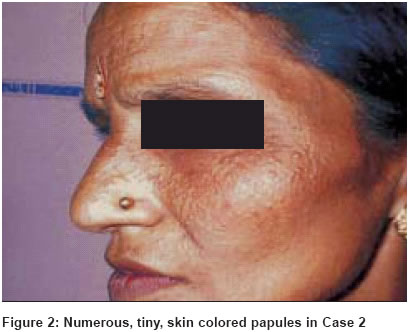
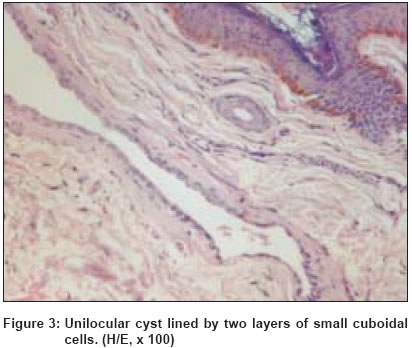
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 6, November-December, 2004, pp. 367-369 Case Report Multiple eccrine hidrocystomas: Report of two cases treated unsuccessfully with atropine ointment Khunger Niti, Mishra Sharmila, Jain RK, Saxena Sunita Department of Skin and STD, V. M. Medical College and Safdarjang Hospital, New Delhi Code Number: dv04126 ABSTRACT Eccrine hidrocystomas are rare, benign, cystic lesions with a lining that resembles that of the eccrine sweat gland and may be solitary or multiple. Multiple eccrine hidrocystomas occur predominantly on the face as asymptomatic, skin-colored to bluish lesions associated with a chronic course and seasonal variability. Treatment of multiple lesions on the face is challenging. Efficacy with atropine ointment is variable. Botulinum toxin and pulsed dye laser are reported to be beneficial. Two cases of multiple eccrine hidrocystomas are reported who showed no response to 1% atropine ointment.KEY WORDS: Eccrine hidrocystoma, Eccrine neoplasms, Topical atropine INTRODUCTION Hidrocystomas are cystic tumors of the skin. They are classified into two types, namely apocrine and eccrine hidrocystomas according to their histological and presumed histogenetic derivation. Eccrine hidrocystomas were first described by Robinson in 1893 in women working in a hot and humid environment and presenting with multiple vesicular lesions on the face.[1] In 1973, Smith and Chernosky[2] described another group of patients who had predominantly solitary or few lesions, the majority occurring in males. These two different types of presentations are called the "Classic Robinson" and "Smith and Chernosky" types of hidrocystomas. CASE REPORTS Case 1 A 36-year-old female, housewife, presented with multiple, tiny, skin-colored discrete lesions on her face. The lesions were present for the last three years, increasing in summer and subsiding in winter. On examination, there were numerous skin-colored shiny vesicles present on the malar area of the face. A few lesions were also present on the nose and forehead [Figure - 1] and [Figure - 2]. The size of the lesions ranged from 1 to 3 mm in diameter. Clear fluid oozed out on pricking the lesions with a sterile needle. Histopathological examination revealed a unilocular well-demarcated cyst in the superficial and mid-dermis. The wall of the cyst was lined by two layers of small cuboidal cells. At places the wall showed only one layer of cells. The overlying epidermis was normal [Figure - 3]. There was no evidence of decapitation secretion. The cyst cavity was empty. PAS-positive and diastase sensitive granules were present within the cytoplasm of the cell lining the cavity. Case 2 The second patient was a 64-year-old housewife who presented with multiple, tiny, shiny, discrete, papulovesicular lesions on the face for the last two years, increasing in summer and reducing in winter. Histopathological examination showed a single cyst cavity in the dermis. The cyst wall was composed of small cuboidal epithelial cells with no evidence of decapitation secretion. In both patients topical 1% atropine cream was used twice a day for two weeks. There was no significant response and the lesions subsided spontaneously as winter set in. DISCUSSION Multiple eccrine hidrocystomas are rare, benign, cystic lesions occurring predominantly on the face, and associated with a chronic course and seasonal variation. Our cases were classical cases of the Robinson type of eccrine hidrocystomas, occurring in housewives exposed to the hot and humid environment of household work in a tropical climate. The cause of multiple eccrine hidrocystomas is not known. Various postulations which lead to retention of sweat are poral closure causing secondary dilatation of the sweat duct, or adenomatous proliferation of the excretory duct.[2] Differentiation from apocrine hidrocystomas poses a problem both clinically and histologically. Apocrine hidrocystomas are often larger, darker blue in color and less likely to be periorbital.[3] They are generally solitary and do not show seasonal changes or become symptomatic in hot weather. On histological examination, eccrine hidrocystomas which are lined by ductal cells differ from apocrine hidrocystomas by absence of decapitation secretion, PAS-positive granules and myoepithelial cells. Eccrine hidrocystomas are generally unilocular whereas apocrine hidrocystomas are usually multilocular.[3] A controversy exists whether multiple eccrine hidrocystomas are a distinct entity or not.[4],[5] Some authors believe that multiple eccrine hidrocystomas of the face are apocrine hidrocystomas where decapitation secretion has been effaced by the pressure of cyst contents. However, in our patients, serial sections did not show decapitation and we believe that our patients represent true multiple eccrine hidrocystoma. Recent reports indicate that apocrine cystadenomas, apocrine hidrocystomas and eccrine hidrocystomas are distinct conditions.[6] Clinically, it is important to differentiate eccrine hidrocystomas from sebaceous and epidermal inclusion cysts, syringomas, milia and pigmented cystic type of basal cell carcinomas.[7] They are cosmetically undesirable as a result of their predominant facial location. The treatment of multiple eccrine hidrocystomas remains a challenge. The effect of atropine is variable[8] and aggressive surgical excision may lead to scarring. A recent report of a patient treated with pulsed dye laser showed favorable results and opens up further avenues of treatment.[9] Botulinum toxin has been recently reported to be effective in the treatment of multiple eccrine hidrocystomas.[10] In our patient topical 1% atropine cream was used twice a day for two weeks without much benefit and the lesions subsided spontaneously as winter set in. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04126f1.jpg] [dv04126f2.jpg] [dv04126f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}