 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
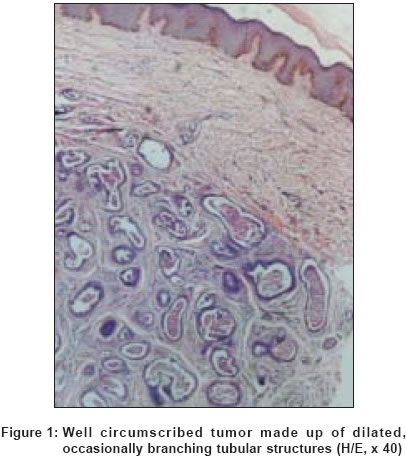
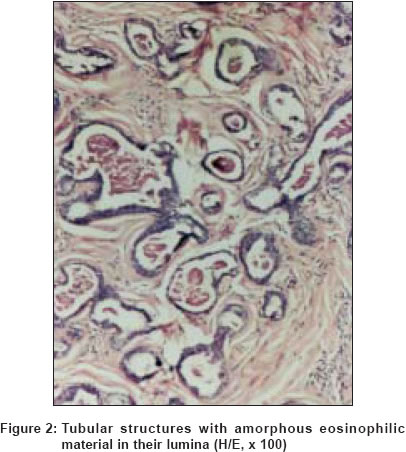
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 6, November-December, 2004, pp. 370-372 Case Report Papillary eccrine adenoma Laxmisha Chandrashekar, Thappa Devinder Mohan, Jayanthi S Departments of Dermatology and STD, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Pondicherry - 605006 Code Number: dv04127 ABSTRACT A 28-year-old man came to us with a solitary skin colored, mildly tender nodule of 6 months duration on the dorsum of the right hand. On histological examination, multiple dilated ducts without apparent continuity with the surface were found in the dermis. These dilated ducts had branching tubules with eosinophilic amorphous material filling most of the lumina. The peripheral cells of the tubules resembled myoepithelial cells, whereas the luminal border cells were cuboidal or low columnar. Papillary projections arising from the inner cells were seen extending into the lumen. These features were diagnostic of a rare tumor, papillary eccrine adenoma.KEY WORDS: Papillary eccrine adenoma; Nodule on hand INTRODUCTION Papillary eccrine adenoma represents the eccrine equivalent of tubular apocrine adenoma.[1] It was first described by Rulon and Helwig in 1977.[2] Clinically, these tumors are most commonly located on the extremities, and less commonly over the trunk or face. Most of these tumors occur as dermal nodules and have been present for several months to years. Since its first report, 33 cases have been reported.[1] We report this tumor in a 28-year-old man for its rarity and unique features. CASE REPORT A 28-year-old man presented to us with a slightly painful swelling of 6 months′ duration over the dorsum of the right hand. On examination, a solitary skin colored, firm, mildly tender nodule of 1 cm diameter was seen on the dorsum of the right hand. It was freely mobile. There were no lesions elsewhere. A provisional diagnosis of leiomyoma cutis was made. The nodule was excised and sent for histopathological examination. On histopathological examination, the epidermis was normal. The lower dermis contained a circumscribed nodule composed of multiple dilated ducts without apparent continuity with the surface [Figure - 1]. These dilated ducts consisted of branching tubules with eosinophilic amorphous material filling most of the lumina [Figure - 2]. The peripheral cells of the tubules were flattened and spindle shaped, resembling myoepithelial cells, whereas the luminal border was composed of cuboidal or low columnar cells. The cellular cytoplasm did not appear granular. Papillary projections arising from the inner cells were seen extending into the lumen [Figure - 3]. The tips of some papillae were floating free in the intraluminal space. The stroma around the epithelial neoplasm was fibrous. No mitotic figures were seen. There was no necrosis of epithelial elements, nor was there any evidence of decapitation secretion. Based on these histopathological features, a diagnosis of papillary eccrine adenoma was made. DISCUSSION Papillary eccrine adenoma represents the eccrine equivalent of tubular apocrine adenoma.[2] Histopathologically, it appears to be composed of multiple dilated ducts of variable size that rarely communicate with the epidermis. Characteristically, they show prominent intraluminal papillae formed by proliferation of the inner layer of cells of the epithelial lining of the ducts. The lumina are filled with an eosinophilic amorphous material. Immunoreactivity for S-100 protein, CEA, and EMA is typically present, consistent with differentiation towards the secretory epithelium of sweat glands. The amylophosphorylase reaction, indicating eccrine differentiation, is prominent, but the reaction with acid phosphatase, an apocrine enzyme, shows practically no staining in the tumor.[3] The differential diagnosis of this tumor includes those cutaneous neoplasms that show the formation of intraductal papillary projections. Aggressive digital papillary adenoma is most difficult to differentiate histologically. It is usually located on the fingers and toes of elderly persons, and has a tendency for local recurrence and deep soft tissue infiltration. It is more infiltrative with a nodular and solid architectural configuration and a mild to moderate degree of atypia with pleomorphism. In general, eccrine carcinomas demonstrate more infiltrative characteristics of growth. Necrosis may be present. Some cases show vascular invasion, perineural invasion, or both. They demonstrate more frequent mitotic figures.[2] Syringocystadenoma papilliferum also shows papillary projections into cystic invaginations, but here the papillae are thicker and lined by glandular epithelium with decapitation secretion. The papillary stroma contains abundant plasma cells.[3] Papillary eccrine adenoma needs to be differentiated from hidradenoma papilliferum, which occurs only in women over the labia majora.[3] It is an apocrine adenoma, which appears as a dermal nodule, surrounded by a fibrous capsule. Within the tumor, both tubular and cystic structures are seen. Papillary folds project into the cystic spaces. They have a connective tissue axis and cells of the luminal area show decapitation secretion.[3] Tubular apocrine adenoma resembles papillary eccrine adenoma.[4] This is a well-defined nodule, which usually occurs on the scalp. Tubular apocrine adenoma has fewer papillary projections and its papillae are usually shorter than those of papillary eccrine adenoma. In addition, the luminal cells show many areas of decapitation secretion. Because of their differences in decapitation secretion, enzyme biochemistry, and electron microscopy, the term tubulopapillary hidradenoma with eccrine or apocrine differentiation was proposed.[4] Papillary eccrine adenoma has a unique histopathological appearance, but sometimes it may be difficult to differentiate from other malignant adnexal neoplasms, leading to excessive surgical procedures.[5] Histopathological differentiating features from adnexal cutaneous carcinomas are its symmetry, perpendicularity of its long axis to the epidermis, and the fact that its fibrous stroma is well separated from the surrounding dermis. For complete resection of a papillary eccrine adenoma without significant damage to neurovascular structures, Mohs micrographic surgery may be employed. [6] This case is presented to highlight the typical histopathology of this rare neoplasm and its close differential diagnoses which otherwise can cause confusion leading to management pitfalls. This is probably the first report of this tumor from India. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04127f3.jpg] [dv04127f2.jpg] [dv04127f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}