 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
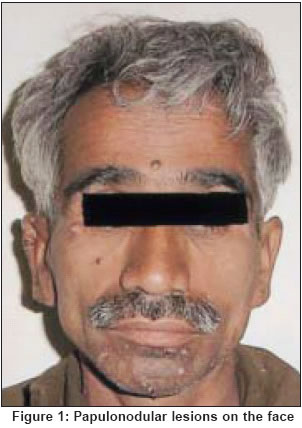
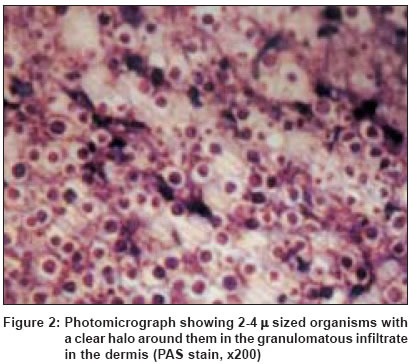
Indian Journal of Dermatology, Venereology, Leprology, Vol. 70, No. 6, November-December, 2004, pp. 391-392 Quiz Asymptomatic nodules over the face Singhi MK, Gupta LK, Bansal Mohit, Garg Dinesh, Purohit SD Department of Dermatology, Venereology & Leprosy, Dr. S. N. Medical College, Jodhpur Code Number: dv04137 A 38-year-old HIV seropositive man from Western Rajasthan had multiple skin colored and erythematous papulonodular lesions on the face, neck and forearm [Figure - 1]. A similar lesion on the forearm also showed central ulceration. He also had generalized lymphadenopathy and mild hepatosplenomegaly. Investigations revealed anemia (Hb: 9.9 gm%, WBC count: 6500/dl, ESR: 90 mm at end of first hour). Stools and urine examination, serum biochemistry and chest X-ray were normal. Ultrasonography of the abdomen revealed mild hepatosplenomegaly with no focal mass. FNAC of cervical lymph nodes revealed chronic non-specific lymphadenitis with no evidence of malignant pathology. The absolute CD4 count was 84. Histopathology of lesions from the forearm and face revealed a granulomatous infiltrate comprising macrophages and lymphocytes. Polymorphs, eosinophils and plasma cells were also scattered within the granulomatous infiltrate. A high power view of granuloma showed numerous 2-4 , oval and round, intracellular as well as extracellular organisms, having a halo around them [Figure - 2]. PAS and Silver methenamine stained the organisms. WHAT IS YOUR DIAGNOSIS? Diagnosis: Disseminated cutaneous histoplasmosis DISCUSSION With the advent of acquired immunodeficiency syndrome (AIDS), histoplasmosis has emerged as an important opportunistic infection among HIV infected persons, usually occurring with a CD4 count less than 75 cells/ìl.[1] Histoplasmosis refers to an infection due to dimorphic fungus Histoplasma capsulatum. Inhalation is the usual mode of infection in humans. The natural habitat of Histoplasma capsulatum is the soil and the fungus has been recovered most frequently from soil enriched with bird or bat droppings.[1] The spectrum of clinical manifestations ranges from asymptomatic illness in normal persons to widespread disseminated infection in immunocompromised individuals.[1] Histoplasmosis is encountered in endemic forms in the USA, Latin America, the Far East and Australia.[2] In these areas, over 70% of adults have been reported to be infected subclinically.[2] In an Indian study from West Bengal, a prevalence of 9.4% has been reported.[3] Despite its endemicity, histoplasmosis is rarely reported from India, perhaps on account of its varied clinical presentation and lack of awareness amongst dermatologists. Panja and Sen first reported histoplasmosis from India in 1959.[4] A few sporadic cases have been reported from South India as well.[5] Recently, we have also reported a case of disseminated cutaneous histoplasmosis successfully treated with itraconazole in an immunocompetent female from North-West Rajasthan.[6] Our patient presented to us in the advanced stage of HIV disease, with a CD4 count of 84. Some cutaneous nodules on the face and forearms were suggestive of giant molluscum contagiosum morphologically. The diagnosis of histoplasmosis was based on histopathology which showed PAS positive, 2-4 sized fungal spores with a clear halo (pseudocapsule). The spores of cryptococcus can be differentiated from those of histoplasma as they are larger (8-12 ) and do not have a well demarcated clear halo. A culture could not be done and no treatment could be given as the patient did not report after the biopsy. Histoplasmosis may present with atypical clinical features in AIDS patients and a high index of suspicion for histoplasmosis should therefore always be kept. Suspected lesions should be subjected to histological examination to ascertain their exact nature. REFERENCES
Copyright 2004 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv04137f1.jpg] [dv04137f2.jpg] |
| |||||||||

{kind=link}
{kind=link}