 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
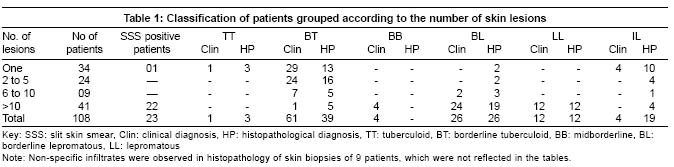
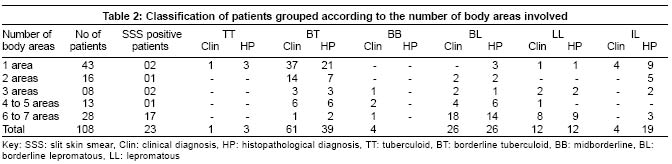
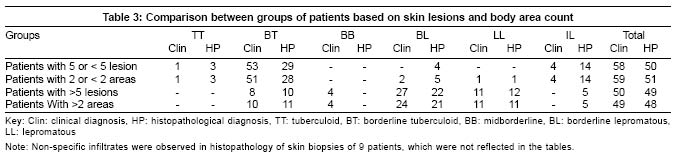
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 14-19 Studies Comparison of two systems of classification of leprosy based on number of skin lesions and number of body areas involved - A clinicopathological concordance study Rao PNarasimha, Sujai Suneetha, Srinivas D, Lakshmi TSS Department of Dermatology, Osmania Medical College, Hyderabad Code Number: dv05001 ABSTRACT BACKGROUND AND AIMS: WHO guidelines classify leprosy patients for therapeutic purposes into paucibacillary (PB) and multibacillary (MB) leprosy based on the number of skin lesions. An alternative system of classification has been in practice in Nepal from 1985 onwards, based on the number of body areas involved in patients of leprosy. We attempted a clinicopathological approach for comparison of these two systems of classification in leprosy patients for their ability to demarcate patients into groups of PB and MB leprosy.MATERIALS AND METHODS: The study included 108 leprosy patients (80 males and 28 females). Complete clinical examination and body charting was carried out in each patient noting the count of skin lesions and the number of body areas involved. Slit skin smears and skin biopsies were taken from an active skin lesion in all patients. RESULTS: On analysis, it was observed that there was good clinicopathological correlation between patients with 5 or <5 skin lesions and 2 or <2 body areas involved. (Clinical 95% and histological 96%) A similar correlation was also observed in the other group of patients with > 5 skin lesions and > 2 body areas involved, (Clinical 94% and histological 96%). There were almost identical numbers of patients represented in these two groups of classification. CONCLUSIONS: Our findings suggest that patients with involvement of 2 or less body areas can be classified as PB leprosy and those with more than 2 body areas involved can be classified as MB leprosy for the purposes of therapy. The study of areas of involvement in leprosy patients not only provides additional patient information but also adds another parameter as a basis for the study of leprosy patients. KEY WORDS: Classification of leprosy, Count of skin lesions, Number of body regions. INTRODUCTION In India and in most endemic countries, for purposes of therapy leprosy patients are classified into paucibacillary (PB) and multibacillary (MB) types on the basis of the number of skin lesions, with five lesions being the determining number.[1] A count of the body areas involved in leprosy is an alternative method of classifying leprosy for therapeutic purposes and is used in leprosy control programs in Nepal.[2] Both methods are based on simple, easily practiced clinical parameters. In the present study we used the clinical diagnosis and skin histopathology based on the Ridley-Jopling classification to compare the validity of these two methods in classifying patients into PB and MB groups and also to find any correlation between these two systems. METHODS The study group consisted of 108 newly registered leprosy patients (80 males and 28 females) who attended the Dermatology OPD of Osmania General Hospital, Hyderabad, India, between January 1998 and December 1999. Patients with all the clinical types of leprosy, except the pure neuritic type, were included in the study after informed consent. Complete dermatological examination was carried out in all patients and the number of lesions recorded and charted. The body surface was divided into seven areas: both upper limbs - 2 areas; both lower limbs - 2 areas, anterior and posterior aspects of trunk - 2 areas; and head and neck - 1 area. The number of areas involved in each patient was counted and recorded, not considering the number of lesions in each area. Each patient was given a score on a scale of 1-7 depending on the number of areas involved. Slit skin smear (SSS) examination was performed on all patients. Skin biopsies were taken from active lesions in all patients and were processed at Dhoolpet Leprosy Research Centre, Lepra India, Hyderabad. They were stained by Hematoxylin and Eosin stain and modified Fite stain and graded as per the Ridley-Jopling classification into indeterminate (IL), tuberculoid (TT), borderline tuberculoid (BT), mid-borderline (BB), borderline lepromatous (BL) and lepromatous leprosy (LL). RESULTS Thirty-four patients had a single lesion of leprosy, 24 had 2-5 lesions, 9 had 6-10 lesions, and 41 had more than 10 lesions. Only one body area was involved in 43 patients, 2 areas in 16 patients, 3 areas in 8 patients, 4 to 5 areas in 13 patients, and 6 to 7 areas were involved in 28 patients. Slit skin smears were positive for AFB in 23 out of 108 (21%) patients, including 22 from BL and LL leprosy patients and in one patient of BT leprosy in type 1 lepra reaction. The highest value of BI was 4+, observed in 6 LL patients. All SSS positive patients had more than 5 skin lesions, except for one patient with BT leprosy in type 1 lepra reaction who had less than 5 lesions. Twenty of the 23 SSS positive patients had more than 2 body areas involved; the remaining three had 2 or less body areas involved. The clinical and histopathological classification of leprosy in patients grouped on the basis of the number of skin lesions is given in [Table - 1]. In patients with a single skin lesion of leprosy, the commonest clinical type was BT leprosy (29 out of 34 patients). However, the histopathological features of BT leprosy were observed in only 13 out of 34 patients of this group, with 10 patients showing features of IL and 2 patients of BL leprosy. In the group of patients with 2 to 5 lesions, all 24 patients were classified clinically as BT leprosy, whereas on histopathology, only 16 out of 24 showed features of BT leprosy. In the 6 to 10 lesions group, the clinical-histopathological correlation was better, with 5 out of 7 BT patients and 2 out of 2 BL patients showing concordance. In the group with >10 skin lesions, 28 out of 41 patients were clinically BB or BL, whereas the histopathology was BL or LL in 31 patients. Please note that non-specific infiltrates were observed in histopathology of skin biopsies of 9 patients, which were not reflected in the results. Similarly, the number of body areas involved correlated with the clinical and histopathological diagnosis [Table - 2]. Forty-two of the 43 patients in whom one body area was involved were clinically diagnosed as TT, BT, or IL leprosy. One patient with involvement of the face and nodularity of the pinna was clinically diagnosed as lepromatous leprosy and this was confirmed by skin smears and histopathology. Three patients in this group had clinical features of BT leprosy but had BL leprosy on histopathology. Good clinicopathological correlation was observed in patients with involvement of 4 to 7 body areas, with concordance in 33 out of 41 patients. Comparisons were drawn between groups of patients based on the lesion count and the groups based on body areas involved [Table - 3]. When the patients were divided on the basis of number of lesions, it was observed that 58 out of 108 patients belonged to the 5 or <5 lesions group and the rest 50 to that with >5 lesions. Similarly, when they were classified based on the body areas involved, 59 patients had 2 or <2 area involvement and 49 patients had >2 body areas involved. When the group of patients having 5 or <5 lesions was compared for clinical and histopathological types with the group having 2 or <2 areas of involvement, the following observations were made. There was a good correlation in the clinical classification (95%) and histopathological typing (96%) between these two groups. When clinical types TT, BT and IL were compared between the two groups, 100% concordance was found in TT and IL leprosy and 96% concordance in BT leprosy. The majority of patients in 2 or < 2 areas group belonged clinically (95%) and histopathologically (88%) to the TT, BT and IL groups (i.e. the paucibacillary forms of leprosy). When the group having more than 5 lesions was compared with the group having 3 or more body areas involvement, predominance of the multibacillary type of leprosy, both clinically (74% and 84% respectively) and histopathologically (65% and 68% respectively), was observed. Overall, the concordance between these two groups was 94% clinically and 96% histopathologically. DISCUSSION The spectrum of disease in leprosy has been characterized in a number of clinico-immunopathological classification systems, the most widely used one being the Ridley-Jopling classification. Since the introduction of WHO multi-drug therapy (MDT), classification of patients simply into PB and MB treatment groups based on the skin smear status has become a normal practice. The WHO has subsequently advocated the classification of patients into PB and MB groups based on the count of body lesions.[1] However, this system has led to a small but significant number of smear positive MB cases being treated with the PB treatment regimen,[3] and is hence far from being perfect. There are other methods of classification of leprosy for treatment purposes which are being practiced based on clinical parameters. Classification of leprosy into PB or MB groups based on the count of body areas has been in use in Nepal since 1985 and was acknowledged by the WHO.[2] The Western and Eastern regions of Nepal use variations of this count of the body areas involved, the former dividing the body into 9 areas and the latter dividing it into 7 areas. Our study has followed the latter method. A study from Nepal has considered the presence of skin or nerve lesions in an area as a sign of involvement,[4] but we have considered only the presence of skin lesions, as the precise definition of nerve lesions or nerve involvement is difficult and is subject to wide observer variability. We observed that when one body area was involved, the clinical diagnosis was always paucibacillary (TT, BT or IL) leprosy, except in one patient who presented with obvious features of diffuse lepromatous infiltration of face and pinna, making the clinical diagnosis of MB leprosy obvious. In a study from Bangladesh 9 out of 89 MB patients presented with involvement of a single body area,[5] whereas in the Nepalese study[4] none of the 31 MB leprosy patients presented with single area involvement. The reason for this marked difference could be due to the higher number of MB patients (173 out of 244) in the Bangladesh study, which probably reflects the type of leprosy prevalent in that part of the world. The sensitivity and specificity of a set of clinical criteria in various studies are stated with reference to the bacteriological status as the gold standard.[6] The WHO system of classifying leprosy patients as MB patients based on number of skin lesions is simple to apply and has a reasonable balance between sensitivity and specificity.[3] In the present study, the number of patients who had 5 or < 5 lesions was almost equal to the number of patients with 2 or < 2 areas involved (58 and 59 patients respectively). However, these groups of patients (with 5 or < 5 lesions and with 2 or < 2 body area involvement) are not a homogeneous group of PB patients but also contain some MB patients as per Ridley-Jopling classification as evidenced by histopathology. Both groups, however, showed good concordance in their clinical and histopathological classifications. Similarly, it was also observed that the number of patients with >5 skin lesions was almost equal to the number of patients with >2 body area involvement (49 and 50 patients). The concordance between >5 skin lesions and >2 body area group of patients was 94% in clinical and 96% in histopathological classifications. Similar observations were made in a study in Bangladesh which found that at least 3 body areas were involved in 100% of patients presenting with 6 or more skin lesions.[5] The authors calculated that if the MB criterion was the presence of 3 body areas affected by leprosy, the sensitivity is 83.1%. In a similar study in Nepal, the criterion of 3 affected body areas in patients in whom skin biopsies were performed, resulted in a sensitivity of 93% for MB leprosy.[4] Various other methods of classification of leprosy for treatment purposes have been evaluated. In a study on Ethiopian patients where the diagnosis of PB or MB was based on skin smears,[7] it was observed that if patients with more than 5 skin lesions were classified as MB, 58% of the patients with negative skin smears, who were actually PB cases, would be overdiagnosed as MB leprosy. The authors argued that with such a degree of MB overdiagnosis, it could rather be advocated that all patients be treated as MB patients for treatment purposes. However, it must be noted that the use of skin smears for the classification of patients into PB and MB groups is no longer followed in most leprosy programs and is not recommended by the WHO.[8] In a trial of a single dose of ROM (rifampicin, ofloxacin and minocycline) for PB leprosy patients with only two or three lesions,[9] when various sub-groups of patients were analyzed, it was observed that in patients with involvement of a single body part, the efficacy of standard WHO-PB MDT was very similar to that of ROM, as judged by its ability to clear lesions. However, when two or more body parts were affected, the difference between the two regimens was significant, with the WHO-PB MDT being superior to ROM therapy. Of the 26 patients with involvement of two or more body parts who were treated by the standard WHO-PB MDT, 13 had complete clearance, compared with only six of the 30 such patients who were administered ROM therapy. These observations suggest that WHO-PB MDT is superior to ROM therapy in patients when two or more body parts are involved. In other words, it is the extent of involvement as assessed by the number of body parts/areas involved (when the total number of skin lesions is constant or the same), which determines the outcome of success of therapy. In this trial, only patients with two or three skin lesions were included and hence a maximum of 3 body parts were involved. However, in PB leprosy patients, a maximum of five body parts could be involved and the study of the relative efficacy of WHO-PB MDT in these patients grouped on the basis of number of body areas involved would be interesting. Leprosy patients have been traditionally classified based on the number and type of skin lesions into various clinical groups. In normal dermatological practice, as in the treatment of diseases such as psoriasis, the extent of body area involved (<20% or >20%) determines the use of specific systemic treatment.[10] A similar logic is used for diseases such as Hodgkin′s lymphoma where the extent of involvement determines the grading of the disease and the therapy.[11] In leprosy, the assumption is that the protective immunity is inversely related to the number of lesions or the number of body areas affected and therefore multibacillary patients have a significantly greater number of lesions or body areas affected than paucibacillary patients.[12] However, as per current WHO guidelines, only the number of skin lesions determines the duration of therapy that patients receive for leprosy. Various studies have reported and highlighted the discrepancies between clinical classification and skin and nerve biopsy findings of leprosy patients.[13],[14],[15], [16] However, the findings based on these observations of skin and nerve biopsies are still to be assigned a decisive role as a basis for therapy. The inferences drawn from the data in the present study are broadly as follows. When one area was involved it almost always was PB leprosy, except when the face was diffusely infiltrated. When two areas were involved, the type of leprosy was most likely to be PB leprosy, with 14 out of 16 patients in this study with involvement of two areas showing clinical and histopathological features of PB leprosy. When 3 or more areas were involved it was predominantly MB leprosy, with 46 out of 49 patients presenting with more than 5 skin lesions. Since the introduction of MDT, many systems and procedures have been simplified so that the general health worker in the field can detect and manage leprosy patients.[12] Classification of leprosy for treatment purposes based on count of body lesions is one such simplification. However, classification of patients into PB and MB groups by count of lesions alone was not perfect as shown in the present study, where 4 out of 58 patients (7%) with 5 skin lesions showed BL on histopathology. Classifying patients by area of involvement alone was also not perfect as there were 6 patients (10%) out of 59 patients with 2 area involvement who showed MB histopathology. Even after combining these two parameters (5 or < 5 skin lesions plus 2 or< 2 area of involvement), there were still 4 patients with histopathology of MB leprosy in this group. If the classification of leprosy for therapeutic purposes is based solely on clinical criteria, it will be useful to combine simple parameters such as the number of skin lesions, the number of areas involved and the size of the area involved. In the present study we have not attempted to measure the area or percentage of body surface involved in these patients. However, such a combined approach for the division of leprosy patients into PB and MB groups is applicable as all health workers, irrespective of the availability of infrastructural facilities, can practice it. Any effort in this direction to make classification of patients into therapeutic groups more comprehensive and precise should be welcome. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05001t3.jpg] [dv05001t2.jpg] [dv05001t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}