 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
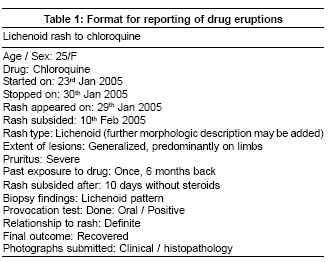
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 1-2 Editorial Reporting of drug eruptions: The national pharmacovigilance program Khopkar Uday Department of Dermatology, KEM Hospital and GS Medical College, Mumbai Code Number: dv05002 In the daily drudgery of clinical practice, every now and then we come across a patient who is sure that a particular drug is affecting his or her skin in a peculiar way. However, to our brains, trained to recognize common drug eruptions, it seems fantastic that any drug could cause side effects such as digitate dermatosis,[1] mycosis fungoides,[2] leukemoid reaction,[3] leg ulcer[4] or even fairness![5] As we understand the myriad ways in which drugs affect the skin, such unusual reactions can be explained with increasing ease. But, to recognize new patterns of adverse drug reactions (a better term than eruptions as there may be no rash) we must increase our index of suspicion, particularly with novel classes of drugs. Drug eruptions can be classified into:[6] definite, if both de-challenge (resolution of rash after drug withdrawal) and re-challenge (oral or patch test, or intradermal test as appropriate) are positive; probable, if only de-challenge is positive but re-challenge is negative or is not done; and possible, if there is only a reasonable time relationship between the drug and the adverse cutaneous event but information on de- or re-challenge is not available or unclear.[6] In India drug reactions are uncommonly reported on a regular basis, except by a few departments of dermatology or pharmacology affiliated to tertiary care centres.[7] Now the infrastructure for reporting them is being put in place. The WHO sponsored and World Bank funded National Pharmacovigilance Program for India will be operational from 1st January 2005.[8] It will be overseen by the National Pharmacovigilance Advisory Committee based at the Central Drugs Standard Control Organization (CDSCO), New Delhi. Two zonal centers, the South-West zonal centre (located at the Department of Clinical Pharmacology, Seth GS Medical College and KEM Hospital, Mumbai) and the North-East zonal centre (located at the Department of Pharmacology, AIIMS, New Delhi), will collate information from all over the country and send it to the Committee as well as to the Uppsala Monitoring centre in Sweden. Three regional centers will report to the Mumbai centre, and two to the New Delhi one. Each regional centre in turn will have several peripheral centres reporting to it. Presently there are 24 peripheral centers. The program has three broad objectives: the short term objective is to foster a reporting culture, the intermediate objective is to involve a large number of healthcare professionals in the systems and information dissemination, and the long term objective is for the program to be a benchmark for global drug monitoring. In order to make the program successful we need to regularly report all drug eruptions to a peripheral or zonal centre using a postal form (http://www.cdsco.nic.in/adr2.pdf). To facilitate reporting of unusual adverse reactions by dermatologists, the IJDVL is planning to publish brief (up to 250 words) reports of reactions as shown in [Table - 1] on the journal web site. Of course the option to submit such reports in the regular letter or case report format for its printed version will be retained. Reactions may also be reported in this format to any peripheral or zonal centre. Only our participation can ensure the success of this program. ACKNOWLEDGMENTS The author is thankful to Dr. Nithya Gogate, Associate Professor, Department of Clinical Pharmacology, KEM Hospital and Seth GS Medical College, Mumbai for her inputs on the National Pharmacovigilance Program. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05002t1.jpg] |
| |||||||||

{kind=link}