 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
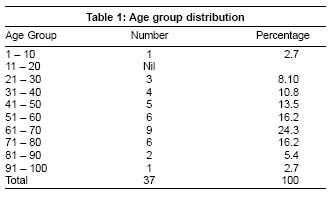
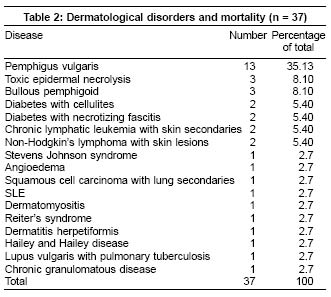
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 23-25 Studies A study of mortality in dermatology Nair PradeepS, Moorthy PrasannaK, Yogiragan K Departments of Dermatology and Venereology, Medical College Hospital, Trivandrum - 695 011 Code Number: dv05004 ABSTRACT BACKGROUND AND AIMS: Certain dermatological conditions are life-threatening and can cause mortality. The aim of this study is to find out the dermatological diseases leading to death in our indoor patients.METHODS: A record-based retrospective descriptive study of dermatology cases who died during the period of 1995 to 2001. RESULTS: The total number of cases analyzed was thirty-seven. There were 24 males and 13 females. The maximum number of deaths occurred in the age group 61-70. Vesiculobullous disorders were the commonest cause of death, found in 18 cases (48.6%), followed by drug reactions in 5 (13.5%), malignancies in 5 (13.5%) and collagen vascular disease in 2 cases ((5.40%). Pemphigus was the commonest fatal vesiculobullous disorder (13 cases - 35.13%), and toxic epidermal necrolysis the commonest drug reaction (3 cases - 8.10%). CONCLUSION: Area of skin involvement, electrolyte imbalance and septicemia were important factors leading to death in pemphigus and toxic epidermal necrolysis. We advocate that such patients should be managed in burns unit or ICU units. KEY WORDS: Dermatology, Mortality. INTRODUCTION There is a belief among the medical fraternity and the general public that dermatological diseases are not life-threatening and cannot kill the patient, which we know is not true. Moreover, there are very few studies worldwide regarding mortality in dermatology. Most of the studies done on mortality have been disease-specific and not general.[1],[2] In India too, no general mortality studies in dermatology have been done, but morbidity related studies have been done.[3] It is a well known fact that there are life-threatening dermatological diseases such as pemphigus, toxic epidermal necrolysis (TEN) and exfoliative dermatitis which in spite of therapy can cause fatalities. In patients with collagen vascular disorders like SLE, systemic organ involvement can contribute to the mortality. Taking these facts into consideration we decided to undertake this retrospective study of mortality in dermatology patients in our wards. METHODS A record-based retrospective descriptive analysis of all the indoor patient case books and death certificates of all patients who died in the Department of Dermatology and Venereology, Medical College Hospital, Trivandrum from 1995 to 2001 was carried out. The records were obtained from the records library of the hospital. The Medical Certification of Cause of Death (MCCD) records were used to obtain data regarding deaths. The data regarding the cause of death were taken from the death certificates as noted by the attending Physician/Dermatologist at the time of death. Since the deaths occurred due to known causes in the hospital wards no post-mortems had been performed. The data regarding the disease and management of the cases were obtained from the inpatient case books. A total of 37 cases were analyzed for the study. RESULTS The total number of patients admitted in the dermatology ward during the study period was 1034. The total number of deaths in the study period was 37. Hence the mortality rate was 3.58%. There were 24 males (64.8%) and 13 females (35.2%). The male/female ratio was approximately 2:1. The age group distribution is given in [Table - 1]. The maximum number of deaths, 9, occurred in the age group 61-70. The youngest patient was 3 years old and the oldest was aged 97. There were no deaths in the age group 11-20. The immediate cause of death in all the cases was cardio-respiratory arrest. The dermatological disorder and related complications were responsible for 30 deaths (81.1%), therapy-related complications accounted for 4 deaths (10.8%) and 3 deaths (8.1%) occurred due to medical complications unrelated to the skin disorder. The dermatological disorders which caused mortality in the study period are given in [Table - 2]. Out of those, vesiculobullous disorders were the commonest cause of death, accounting for 18 cases (48.6%), followed by drug reactions in 5 (13.5%) and malignancies in 5 (13.5%). Among the vesiculobullous disorders, pemphigus vulgaris was the commonest, accounting for 13 cases (35.13%). Of these, 7 cases were males and 6 females. Their age varied from 43 to 97 years. Four cases had concomitant diabetes. TEN was the commonest drug reaction to cause death in 3 cases (8.10%). The malignancies causing death were chronic lymphatic leukemia (CLL) in 2 cases (5.40%), 2 cases of non-Hodgkin′s lymphoma (5.40%) and 1 case (2.70%) of squamous cell carcinoma with lung secondaries. DISCUSSION The mortality rate of 3.58% in this case series may indicate a relatively low rate considering the fact that only serious patients are admitted to the dermatology wards. But no definite inferences can be made as there are no comparable mortality studies in dermatology from other parts of the India. The maximum number of deaths occurring in the age group 61-70 is in general concordance with other studies as it is well known that old age contributed to mortality in diseases like pemphigus, TEN and malignancies. Pemphigus vulgaris was the commonest disorder to cause death in this study. All these patients had severe oral lesions. Ten patients had skin involvement greater than 70% and 3 patients had skin involvement greater than 90%. Extensive skin involvement, septicemia, bronchopneumonia and electrolyte imbalance were the causes of death in these patients. Mortality studies done for pemphigus elsewhere indicate rates of 5-15%.[1],[4] These studies were done in advanced centers of the world where the patients were managed in burns and ICU units which could explain the relatively low mortality rate. This may not be possible in India as surgical and medical emergencies are given priority in the burns and ICU units. Another important feature noted in our study was that 10 cases of pemphigus died during the period of 1995 to 1998, while from 1999 to 2001 there were only 3 deaths. This is due to the fact that from 1999 onwards our department initiated Dexamethasone-Cyclophosphamide pulse therapy (DCP) for pemphigus patients which is well known to reduce the morbidity and mortality in such patients.[5] TEN accounted for 8.10% of the mortality with carbamazepine as the cause in all the cases. All these patients had involvement of body surface area in excess of 90% with ocular, oral and genital involvement. The mortality rates for TEN from other studies range from 10-70%.[6] Low mortality rates have been reported from centers where the patients were treated in the burns ward.[7] The 2 cases of CLL had skin secondaries in the form of papules and nodules. The presence of secondaries in any malignancy usually increases the mortality rate.[8] Severe anemia and chemotherapy-induced toxicity contributed to the mortality in these cases as well as in the cases of non-Hodgkin′s lymphoma. Two diabetic patients in the study had developed necrotizing fasciitis which contributed to the mortality. The patient with SLE had renal involvement and acute renal failure was the cause of death. Renal involvement is known to increase the mortality in SLE patients. [9]The case of Hailey and Hailey disease and one case of bullous pemphigoid died due to complications of immunosuppressive therapy. In 3 cases the cause of death was unrelated to the dermatological condition. The patient of dermatitis herpetiformis died due to atrial fibrillation, lupus vulgaris due to myocardial infarction and Reiter′s syndrome due to paralytic ileus. This case series is a record-based study which has inherent limitations. The sample size is also small. However, we would like to highlight in this study that the area of skin involvement, septicemia and electrolyte imbalance were important factors which contributed to the mortality in pemphigus and TEN cases. Barrier nursing is very important in cases where extensive skin tissue is lost. Hence we advocate that patients with pemphigus and TEN should be managed in burns units or ICU units if possible, where superior medical and nursing care can be given. This will definitely reduce the mortality of these dreaded disorders. Since immunosuppressive therapy was another factor contributing to mortality we should be cautious and selective in starting this potent group of drugs in patients after carefully weighing the risk-benefit ratio. To the best of our knowledge this study of mortality in dermatology is the first of its kind to be conducted in India. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05004t2.jpg] [dv05004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}