 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
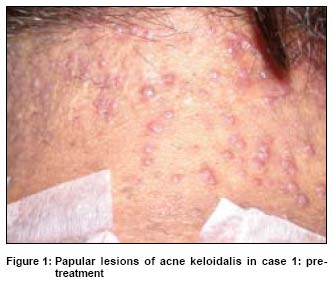
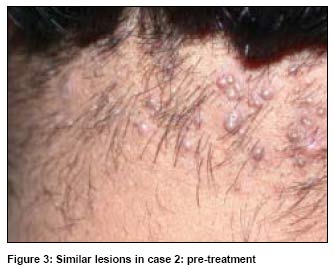
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 31-34 Case Report Efficacy of diode laser for treating acne keloidalis nuchae Shah GirishK Consultant dermatologist, Mumbai Code Number: dv05006 ABSTRACT Acne keloidalis nuchae is usually treated with oral antibiotics, local antiseptics or intralesional steroids but with limited success. I assessed the efficacy of diode laser for treating the inflammatory and keloidal papules of acne keloidalis nuchae in two cases. The lesions in both the cases showed about 90 to 95% clearance after 4 treatment sessions at one to one and half month intervals. No new lesions were observed during the follow up period of six months after the last laser treatment. Thus, after clearing bacterial infection, laser hair epilation can be used as the first line of therapy for treating papules of acne keloidalis nuchae. This is the first attempt at treating acne keloidalis nuchae with a diode laser. KEY WORDS: Acne keloidalis, Diode laser. INTRODUCTION Acne keloidalis nuchae (AK), also known as folliculitis keloidalis, is a chronic inflammatory process involving the hair follicles of the nape of the neck. It is characterized by the presence of papules and pustules arranged in irregularly linear groups just below the hairline. The disease persists for many years as new papules continue to form at intervals and they heal leaving behind hypertrophic or keloidal papules. Many treatment modalities like oral and local antibiotics and intralesional steroids have been used to treat this condition but with limited success. In severe cases surgical excision or carbon dioxide laser ablation followed by healing by secondary intention have been tried with some success. Early lesions of AK show a follicular and perifollicular infiltrate at the upper one-third of the hair follicle on histopathology, while advanced lesions show a granulomatous infiltrate around broken hair fragments. Hence any treatment that destroys the hair follicle is likely to improve this condition. The use of laser hair epilation is widely recommended for chronic follicular inflammatory conditions like pseudofolliculitis barbae. Hence I decided to use a diode laser for the reduction of terminal hair in patients with AK. I describe two patients whose papules of AK were treated effectively with the diode laser. CASE REPORTS Patient 1 A 50-year-old school principal presented at my clinic with papules and nodules on the nape of the neck of 3 years′ duration [Figure - 1]. A diagnosis of AK had been made 3 years earlier based on the clinical and histopathological findings. The patient had taken many oral antibiotics for prolonged periods and had also received 6 intralesional triamcinolone injections about 6 months back without any benefit. He had not received any treatment for the past 6 months. On examination, multiple small follicular papules were seen on the nape of his neck. Some were small and fleshy while others had a keloidal appearance. On the basis of the clinical and histopathological findings the skin condition was confirmed as AK. Patient 2 A 36-year-old businessman visited my clinic with a complaint of many painful papules and nodules on the nape of the neck of 2 years′ duration [Figure - 2]. He had been diagnosed as a case of AK on clinical grounds and had been treated with oral antibiotics and topical tretinoin 0.025% cream for 10 months. He had also received 3 intralesional injections of triamcinolone acetonide 10 mg/ml at monthly intervals during these 10 months. He had discontinued all treatments as he had continued to develop new papules and nodules. On examination he had multiple papules on the nape of the neck. Most of them were smooth and fleshy while a few showed keloidal changes. On clinical grounds he was diagnosed as AK. Both patients were treated with laser hair epilation with the diode laser (LightSheer diode laser, Lumenis Inc. USA). The treatment was started after seven days of oral antibiotics. All hair on the nape of neck were closely trimmed. The first and second treatments were given at 23 fluence and 100 ms pulse width while the third and fourth treatments were given at 26 fluence and 100 ms pulse width. After each treatment the patients were given ice compresses for 10 minutes and were advised to use a sunscreen with SPF 30 during the daytime and topical tretinoin cream 0.025% combined with betamethasone dipropionate cream 0.05% at night. Treatment was repeated at 4-6 week intervals for 4 sittings. Pre-treatment and post- treatment photographs were taken during each visit. Patient 1 had 95% clearance [Figure - 3] and patient 2 had about 90% clearance [Figure - 4] of papules in the nape area one month after the fourth treatment. A few fine, soft hairs were present in both patients after 1 month of the last treatment while grey colored hair persisted in patient 1 at the end of 4 treatments. Patient 2 had burns at the site of treatment but this subsided within 7 days. Both patients had no other side effects like hypo- or hyperpigmentation. The papules decreased in number and reduced in size as the hair grew thinner with each treatment. No new lesions appeared once the treatment was initiated or even during the 6 months period after the last treatment. DISCUSSION AK is characterized by the occurrence of keloidal follicular papules and plaques on the nape of the neck, especially in black males. While the exact cause of AK is not yet known, frequently suggested etiological possibilities are short haircuts along the posterior hairline and penetration of cut hair into the skin, as in pseudofolliculitis,[1] constant irritation by shirt collars,[2] and chronic low-grade bacterial infection.[2] Sperling et al suggest that AK is a primary form of scarring alopecia.[3] Histologically, there is a follicular and perifollicular infiltrate at the upper third of the hair follicle. A more advanced lesion shows rupture of the follicle and the development of a granulomatous infiltrate around a broken hair fragment.[4] The lower portion of the follicle is not affected until the later stages of the disease and these hair continue to proliferate beneath fibrous tissue, producing multiple fragments that are seen late in the lesions.[4] A foreign body response continues around these hair follicles. Different medical treatments like broad-spectrum antibiotics, oral and intralesional steroids and topical retinoic acid combined with a class 2 or 3 corticosteroid cream have been used with disappointing results. Although surgical treatment, like excision followed by secondary intention healing, gives cosmetically acceptable results,[5] it has a long recovery period. Laser therapy with carbon dioxide has been tried with some success.[6] The diode laser works on the principle of selective photothermolysis.[7] It emits the 810 nm wavelength that is well absorbed by the melanin present in hair follicles and hair shafts. Delivery of high fluences combined with a proper pulse width leads to a rapid rise of temperature and subsequent heat transfer to adjacent tissues. A rise of temperature above 70° C causes necrosis of the follicles′ regenerative structures.[8] Our patients of AK treated with the diode laser showed a gradual decrease in the size and number of papules. This improvement was associated with transient but total loss of terminal hair in the occiput and then growth of hair that were thinner and softer than the original hair. At the end of six months of starting treatment both our patients had cosmetically acceptable results. Though laser treatment in dark skinned individuals can cause pigmentary changes, none of our patients had long term pigmentary changes. The improvement observed following laser hair epilation is probably because of coagulation necrosis of the viable hair follicles and fragmented hair shafts present in the deep dermis. As the hair becomes thinner and softer following laser hair epilation, it loses its strength to penetrate the skin and hence the number of new eruptions decreases. As the healing process in AK is regarded as hypertrophic scarring rather than keloidal,[9] one would expect improvement in the scar once the fragmented hair are removed from the inflammation site. We did not observe any new lesions probably because regrowing hair were thin and soft. Laser hair epilation is a relatively painless procedure and requires no post-procedure care. There are hardly any side effects associated with laser treatment and it gives cosmetically acceptable results. Though laser hair epilation treatment has been used successfully by several workers in the treatment of pseudofolliculitis barbae,[10],[11] there are no reports of its use for the treatment of AK. The pulse dye laser has been used in treatment of keloids and hypertrophic scar, [12] but not for AK. This is probably the first report that the principle of laser hair epilation has been applied in the treatment of AK in patients with skin type IV and V. Hence I suggest that laser hair epilation should be considered as the first line treatment for AK, a condition otherwise difficult to treat. Treatment should be started as early as possible to avoid the morbidity associated with late stage disease. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05006f4.jpg] [dv05006f1.jpg] [dv05006f3.jpg] [dv05006f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}