 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
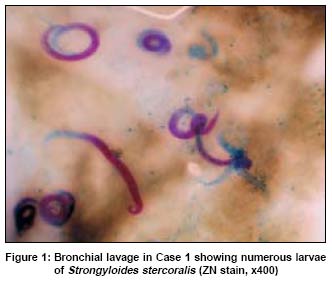
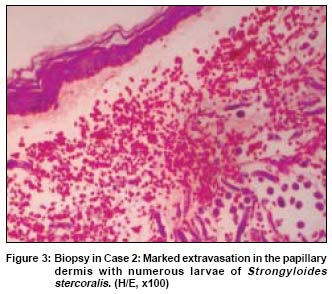
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 38-40 Case Report Fatal disseminated strongyloidiasis in patients on immunosuppressive therapy: Report of two cases Reddy IS, Swarnalata G Departments of Dermatology, Apollo Hospitals, Hyderabad Code Number: dv05008 ABSTRACT Disseminated strongyloidiasis is a rare manifestation in patients on immunosuppressive drugs. We report two cases of fatal disseminated Strongyloides stercoralis infestation. The first was in a patient of pemphigus vulgaris who developed an exacerbation of symptoms, one year after diagnosis and was given intravenous dexamethasone and azathioprine and in the third week of hospitalization developed features of septicemia, respiratory failure and petechial hemorrhages which were proven to be due to disseminated strongyloidiasis. The second patient was diagnosed to have stage IV diffuse large cell type of non-Hodgkin lymphoma and after the second cycle of chemotherapy, developed generalized symptoms of septicemia, respiratory failure, purpuric macules and patches. This was also proven to be disseminated strongyloidiasis.KEY WORDS: Disseminated strongyloidiasis, immunosuppression. Strongyloides stercoralis is distributed worldwide in the tropics and subtropics.[1] The adult female lives in the small intestine. In the majority of patients the parasite load is low and the patient is free of any symptoms. Corticosteroid therapy and malnutrition may change the host-parasite relationship and result in hyperinfection and dissemination.[2] Apart from corticosteroids and malnutrition, other factors for immunosuppression such as leprosy, tuberculosis, malignancy and chemotherapeutic agents may also play a role in dissemination. Though systemic corticosteroids and antineoplastic drugs are used in the treatment of various malignancies, the occurrence of fatal hyperinfection due to strongyloides is rare.[3] Nevertheless disseminated infection carries increased morbidity and mortality.[4] We describe the occurrence of disseminated strongyloidiasis in two patients on immunosuppressive therapy. CASE REPORT Patient 1 A 53-year-old man with pemphigus vulgaris of one year′s duration was hospitalized for acute exacerbation of cutaneous and oral mucosal lesions. Treatment with intravenous dexamethasone 4 mg 8-hourly was started. Azathioprine 100 mg/day was added in the second week. During the third week of hospitalization, the patient developed diarrhea and vomiting which improved with symptomatic treatment. Subsequently he developed headache, drowsiness, breathlessness and hypotension and was shifted to the intensive medial care unit where he developed acute respiratory distress syndrome and became deeply comatose. He was put on ventilatory support. An X-ray chest showed extensive bilateral bronchopneumonia. Secretions from the tracheostomy tube were sent for bacterial and fungal studies. Ziehl-Neelsen stain of bronchial secretions showed numerous larvae of Strongyloides stercoralis [Figure - 1]. A direct wet mount of secretions also showed numerous larvae. Dexamethasone was gradually tapered and stopped, as was azathioprine. The patient was given ivermectin 9 mg/day and mebendazole 100 mg twice daily. On the third day of his stay in the intensive care unit, the patient developed multiple, non-palpable petechial hemorrhages around the umbilicus, lower abdomen and thighs [Figure - 2]. A skin biopsy of the petechial eruption showed dense hemorrhage in the upper dermis, eosinophilic fibrinoid deposits in the vessel walls with occasional lymphomononuclear cells. Scattered strongyloid larvae were seen in the dermis and subcutis without any surrounding inflammatory reaction. The urine sediment also showed a few larvae. The cerebrospinal fluid did not show any larval forms. In spite of one week′s treatment with ivermectin, mebendazole, antibiotics, dopamine, continuous ventilatory support, and nutritional supplementation, the patient died 5 weeks after hospitalization. Patient 2 A 63-year-old man presented with a 5x3 cm sized swelling over the right side of the chest with enlarged lymph nodes in the axillae and inguinal area. Diffuse large cell type of non-Hodgkin′s lymphoma, stage IV was diagnosed. Two cycles of chemotherapy with intravenous vincristine, adriamycin and cyclophosphamide, and oral prednisolone were given. One week after the second cycle of chemotherapy the patient developed fever, dyspnea and abdominal distension. Subsequently, he developed drowsiness, disorientation, worsening of dyspnea, hypotension and purpuric macules and patches over the upper thigh. In view of his abnormal blood gases, the patient was shifted to the medical intensive care unit and put on ventilatory support. An X-ray chest showed bilateral bronchopneumonia. A wet mount of secretions collected from the endotracheal tube showed a few live as well as dead larvae of Strongyloides stercoralis. Skin biopsy of purpuric macules over the thighs showed hemorrhages in the papillary dermis and numerous larvae of Strongyloides stercoralis in the mid dermis [Figure - 3]. The patient was started on ivermectin 6 mg/day and tablet mebendazole 100 mg twice daily. In spite of ventilatory support, antibiotics, dopamine and dobutamine, he died two weeks after hospitalization. DISCUSSION Strongyloides stercoralis is a nematode which is unique because of its ability to complete its life cycle in humans. Chronic bowel infestation may persist for many years without any symptoms. In disseminated strongyloidiasis the larvae enter the lungs, liver, spleen, heart, lymph nodes and esophagus. Dissemination is due to augmentation of the normal life cycle of the nematode which causes a heavy worm burden.[5] Strongyloides stercoralis causes morphologically variable skin lesions.[6] Ground itch is due to penetration of skin by filariform larvae. It manifests as severe pruritus associated with an erythematous papular and papulovesicular eruption most commonly on the feet. In larva currens the larva moves rapidly in the dermis, which results in itchy, serpiginous wheals over the buttocks, groins and trunk. Urticaria, both an acute, generalized form and a chronic form with fixed wheals lasting for one to two days, on the waist and buttocks is also a feature in strongyloidiasis. Rarely, a petechial purpuric eruption which resembles multiple thumb prints may initially present over the periumbilical area.[7] Later on it may involve the whole abdomen, thighs, legs and arms.[8] As observed in our patients, petechial purpuric skin lesions in disseminated strongyloidiasis are due to damage to the blood vessels caused by larval migration. Histopathological studies in our patients did not show any granulomatous response which supports the hypothesis that these patients lack a cell mediated immune response. Various dermatological conditions such as pemphigus and systemic lupus erythematosus treated with immunosuppressives have resulted in fatal hyperinfection with Strongyloides stercoralis.[9],[10] Patients with malignant lymphoma on chemotherapy are also at an increased risk of this serious complication.[11] Since disseminated strongyloidiasis is asymptomatic in the majority of individuals examination of the stool sample of all patients on long term immunosuppressive therapy should be mandatory to prevent the disease′s morbidity and mortality. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05008f1.jpg] [dv05008f3.jpg] [dv05008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}