 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
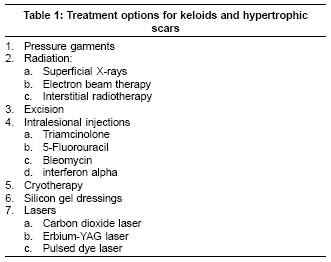
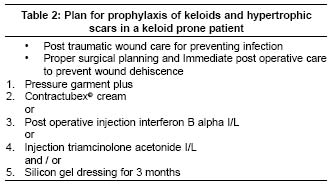
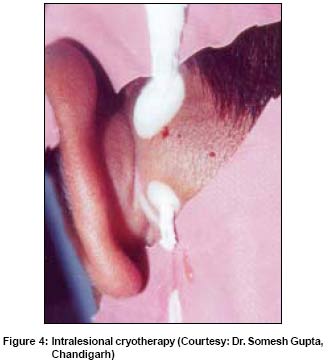
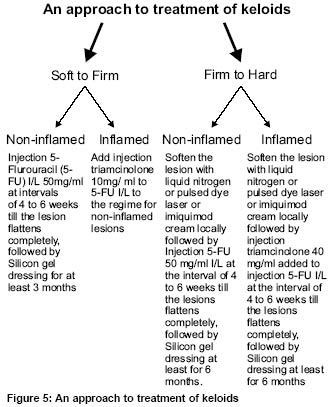
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 3-8 Review Article Treatment of keloids and hypertrophic scars Mutalik Sharad Dermatotherapy and Cosmetology Center, Maharashtra Medical Foundation, Pune Code Number: dv05009 ABSTRACT Clinicians always find it difficult to treat hypertrophic scars and keloids. Various treatment modalities are available. Intralesional corticosteroids, topical applications, cryotherapy, surgery, laser therapy, and silicone sheeting are the widely used options. Radiation therapy can also help in cases of recalcitrant keloids. Most recently, pulsed-dye laser has been successfully used to treat keloids and hypertrophic scars. There are no set guidelines for the treatment of keloids. Treatment has to be individualized depending upon the distribution, size, thickness, and consistency of the lesions and association of inflammation. A combination approach to therapy seems to be the best option.Key Words: Keloid, Hypertrophic scar, Therapy, Prevention. INTRODUCTION Hypertrophic scars and keloids may follow local skin trauma or inflammatory skin disorders like laceration, tattoos, burns, injections, ear-piercing, vaccination, bites, acne, abscess or surgery. They are the consequences of uncontrolled synthesis and deposition of dermal collagen. Experimental evidence implicates the importance of members of the transforming growth factor β(TGF-β) family in cutaneous scarring, as well as scarring in other organs.[1] Virtually every cell in the body, including epithelial, endothelial, hematopoietic, neuronal, and connective-tissue cells, produces TGF- β and has receptors for it. TGF- β regulates the proliferation and differentiation of cells, embryonic development, wound healing, and angiogenesis. TGF- β directly stimulates angiogenesis in vivo. TGF β is released by platelets at the site of injury. Aberrations in the levels of cytokines, including interleukins 6, 13 and 15 may also have a role in keloid formation.[2] Although TGF- β is essential for wound healing, overproduction of TGF- β can result in excessive deposition of scar tissue and fibrosis. A keloid extends beyond the borders of the original wound, does not regress spontaneously, grows in pseudotumor fashion with distortion of the lesion and tends to recur after excision. Whereas hypertrophic scars remain confined to the borders of the original wound and most of the times retain their shape. In hypertrophic scars, collagen fibers are oriented somewhat parallel to the long axis of the scar, on the other hand in keloid, collagen is arranged in completely haphazard manner with presence of keloidal collagen bundles. Anatomically predisposed sites for keloids are shoulders, sternum, mandible and arms (due to increased skin tension at these sites). They are more commonly observed in Asians and dark skinned races.[3] The basic cause of this abnormal wound healing still remains unknown. Medical advice is sought for relief of pruritus, pain, restricted movement and mainly for cosmetic disfigurement. Treatment modalities for keloids and hypertrophic scars include compression garments, radiation, excision, intralesional injections, cauterization, cryotherapy, laser surgery, and silicon gel dressings [Table - 1]. It is difficult to assess the efficacy of the existing treatment modali-ties due to lack of controlled, comparative studies. PREVENTION The first step in minimizing scarring should be attention to the early care of wounds. Following recommendations are based on general principles of wound healing [Table - 2]. The goal with minor wounds such as abrasions is to achieve rapid epithelization by moist healing with ointment or semiocclusive dressings. When epithelization is delayed beyond 10-14 days the incidence of hypertrophic scarring goes up dramatically.[4] Surgical closure of an open wound should take into account the tension on the wound. Wounds subjected to tension due to motion, body location, or loss of tissue (after excision of a lesion) are at increased risk of scar hypertrophy and spreading. Appropriate splinting of the tissue with permanent intradermal sutures should be considered. A useful technique is a subcuticular closure with a polypropylene suture that can be left in place for six months.[5] PRESSURE GARMENTS Prolonged pressure on the hypertrophic collagen has been reported to be effective in preventing recurrence of keloid after surgical treatment.[3] Garments made up of elasticized material are available for different anatomical areas of the body. Such garments are advised immediately after wound healing. RADIATION Superficial x-ray, electron beam therapy and interstitial radiotherapy have been used in the past for effectively treating keloids. There has been controversy in using potentially harmful radiation therapy to treat benign lesions like keloids. But it has been found that good clinical response can be achieved without harmful effects.[3] EXCISION Keloids can be excised with scalpel or electro surgery or laser surgery, but almost 100 per cent keloids are known to recur after surgical treatment. Keloids over areas like ear lobes are less likely to recur after surgical treatment provided proper precautions and post-op treatment is followed. Ideally surgical excision of keloid should be avoided as far as possible, because the failure rate is significantly high. Surgical excision of hypertrophic scars may be efficacious in selected cases but requires meticulous adherence to the surgical principles and adjunctive measures like radiation, intralesional interferon or topical imiquimod.[5] INTRALESIONAL INJECTIONS Triamcinolone Intralesional injection of corticosteroid (triamcinolone acetonide 10 mg / 40 mg) has always remained the first line treatment for keloids. Steroids are known to inhibit collagen synthesis and possess anti-inflammatory properties. Atrophy, one of the side effects of steroids, is utilized to achieve therapeutic effect in keloids. Multiple injections in the keloid bulk at intervals of 4 to 6 weeks are required to achieve desirable effect. Very often it is difficult to force the injection into the hard mass of keloid. This problem could be overcome by softening the lesion either with cryotherapy, or pulsed dye laser or by addition of hyaluronidase, or topical application of immuno-modulator like imiquimod.[6] Adverse sequelae like hypo or depigmentation [Figure - 1], telangiectasia and atrophy are seen in about 20% of cases injected with triamcinolone as reported by Manuskiatti and Fitzpatrick.[7] Berman et al evaluated 13 keloids after surgical excision followed by imiquimod application initiated the night of surgery and continued for 8 weeks. Of the 11 keloids evaluated at the 24 weeks follow - up visit, there were no recurrences observed.[8] 5-Fluorouracil Fitzpatrick has also reported his 9 years experience of using a pyrimidine analog with antimetabolite activity, 5-flurouracil (FFU) 50 mg/ml with or without triamcinolone acetonide, in the treatment of keloids and hypertrophic scars.[9] FFU has been shown to inhibit fibroblast proliferation in tissue culture, and is believed to reduce post-operative scarring by decreasing fibroblast proliferation. Frequent initial injections (once to thrice weekly), followed by injections at intervals of 4 to 6 weeks was found to be effective in reducing the size of the lesions substantially. Interval between 2 injections should be decided by judging the induration and inflammation of the lesions. FFU injections are quite painful. This pain can be alleviated either by addition of triamcinolone acetonide or by giving a field block anesthesia. Addition of 0.1 ml of triamcinolone acetonide (10 mg/ml) to 0.9 ml of FFU (50 mg/ml) helps to reduce the pain and also the inflammation. This mixture should be injected only in the indurated portions until slight blanching is observed. On an average 5 to 10 injection sessions are required to achieve complete flattening of the lesions. Subjective improvement in the form of decrease in pain, pruritus, stretching or pulling sensation, and discomfort is first noted followed by softening and then flattening of the lesion [Figure - 2a and 2b]. The only side effects seen with FFU injection are pain and stinging, blackish discoloration [Figure - 3], purpura at injection site, and occasionally superficial ulceration. Bleomycin Bleomycin in the dose of 1.5 IU/ml injected intralesionally through multiple pricks resulted in flattening of lesions in 6 out of 13 cases.[10] Similarly bleomycin has also been tried by Badokh and Brun intralesionally (0.1 to 1ml at monthly interval) to treat keloids,[11] but its use is restricted due to its side effects and the cost. Antiarrhythmic agent verapamil, which has a property of inhibiting endothelial growth factor and interleukin-6, has been reported in few sporadic trials, to be effective in the treatment of keloids when administered intralesionally.[12] Interferons Interferon α-2b, which has antiproliferative properties, was tried by Berman and Duncan.[13] They injected a keloid intralesionally with 1.5 million IU IFN α-2b, twice over 4 days. The area of the keloid was found to be reduced to 50% of its size by day 9. IFN α-2b, when used post-operatively, reduced the rate of recurrence to 19% as compared with that of intralesional steroid, where the rate of recurrence was 51%.[14] Cryotherapy Freezing the lesions of keloid with liquid nitrogen (LN), with 15-30 seconds freeze-thaw cycles resulted in flattening of those keloids < 6 mm in depth, and lesions over back showed better results as compared to those over chest.[15],[16] Cryotherapy helps to soften the lesions, making the intralesional administration of medication easier. Cryotherapy is quite painful and demands infiltration of local anesthesia. As the freezing effect of spray technique does not reach the entire depth of thick keloids, intralesional cryotherapy has been tried [Figure - 4] and seems to be more effective. It is also devoid of residual depigmentation, commonly observed with spray technique, as the epidermis remains untouched. Because the depth of penetration of the probe technique is 2 cm while the spray technique is even less, lesions 2 cm or more in thickness are difficult to treat by either technique. A therapeutic effect at a depth of 2 cm or more is easy to achieve by the intralesional cryotherapy.[17] Twelves cases of bulky keloids unresponsive to intralesional steroid injections were treated with intralesional LN cryotherapy. A wide bored spinal needle is inserted into the keloid parallel to the skin surface, and the nozzle of the cryo-gun is connected to this needle, for delivering LN. After this therapy seven cases out of 12 showed 75% flattening.[18] For a wider lesion, multiple hypodermic needles are inserted at right angles to the length of the lesion, and LN is delivered through these needles to cover the entire lesion uniformly. Intralesional cryotherapy can cause extensive destruction of the tissue at the point of entry of the needle and its exit. It is a potential hazard if the needle remains in contact with the skin after its introduction into the lesion.[19] This can be avoided by using peripherally insulated needles.[18] It is advisable to restrict cryotherapy to only small keloids.[20] LASERS Ample reports have documented the use of CO2 or Erbium YAG laser for ablating the keloid lesions, but similar to the excision modality, the failure rate is 100%, as the laser ablation actually burns the lesion. Lately pulsed dye laser (PDL) has been tried successfully for softening the lesions. As the target chromophore for PDL is hemoglobin, PDL also helps to destroy the blood vessels supplying the keloid, thereby reducing its size. It has been hypothesized that laser induced tissue hypoxia leads to decreased cellular function, laser induced heating leads to disulfide band disruption with subsequent re-modelling of the fibers, or collagenolysis occurs following cytokine stimulation.[2] Sixteen adult patients with hypertrophic or keloidal median sternotomy scars after heart surgery treated with PDL every 6-8 weeks for 6 months, showed a significant improvement in erythema, scar height, skin surface texture, and pruritus in laser-treated scar areas; this improvement persisted for at least 6 months.[21],[22] SILICON GEL DRESSINGS Silicon gel dressings kept in contact with the keloids, secured with micropore tape, for 12 hours a day, resulted in moderate improvement in 50% cases, within a span of 3 to 6 months.[23] This dressing can also be used as a preventive method immediate post-operatively, after the surgical wound has healed. Of all non-invasive treatment modalities the use of continuous pressure and occlusive contact media, e.g. silicones, seem to be generally accepted as the only ones that are able to manage hypertrophic scarring without significant side-effects.[24],[25] CONCLUSION Even though several modalities of treatment are available for managing keloids, none of the treatments is effective in all patients. Morever, there are no guidelines available. Combination therapy with (1) intralesional 5-flurouracil with or without steroid, (2) pre treatment with intralesional cryotherapy or pulsed dye laser for softening the lesion and reducing the bulk and (3) silicon gel sheet dressing for preventing the recurrence seem to offer better efficacy as compared to any single treatment [Figure - 5]. Immediate post operative intralesional interferon α-2b also helps in preventing the recurrence.[26],[27] FUTURE Multiple treatments have been proposed, often backed by anecdotal evidence alone. Some treatments, such as topical vitamin E, have been widely promulgated as effective in the popular press, whereas others have been marketed directly to the consumer despite a lack of evidence. A number of different approaches have been taken to modify activity of transforming growth factor β locally.[28] The other principal strategy being followed up by pharmaceutical companies is to interfere with collagen synthesis locally, and this has been effective in an animal model. [29] Regardless of the technique employed, an observation period of at least 2 years is necessary to watch for a recurrence.[26] REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05009f2a.jpg] [dv05009f2b.jpg] [dv05009f1.jpg] [dv05009f4.jpg] [dv05009t1.jpg] [dv05009f3.jpg] [dv05009f5.jpg] [dv05009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}