 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
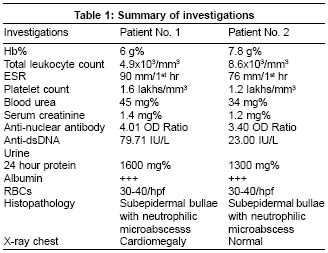
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 54-56 Letter To Editor Bullous systemic lupus erythematosus: Response to dapsone in two patients Sirka CS, Padhi T, Mohanty P, Patel DK, Parida PR, Kar CR Departments of Skin and VD, VSS Medical College, Burla, Orissa Code Number: dv05019 Sir, Bullous systemic lupus erythematosus (SLE) is a transient autoimmune bullous disease that occurs in established cases of SLE. Some authors use this term for all subepidermal autoimmune bullous conditions in SLE, whereas others use it for conditions where dermal antigens are involved.[1] Histopathologically, this condition is characterized by subepidermal bullae with neutrophilic microabscesses, nuclear dust and fibrin at the tips of dermal papillae. Direct immunofluorescence reveals a linear deposition of IgG, IgA, IgM and C3 in the basement membrane zone. The target antigen is believed to be type VII collagen in the dermis. We came across two cases of bullous SLE at our institute. An 18-year-old female presented with arthritis of both knee and ankle joints since the last 1 month, fever since 15 days, oral ulcerations since 10 days, and lacrimation and irritation of the left eye since 4 days. After 3 days of hospitalization, she developed asymptomatic erythematous, non-itchy, maculopapular rash over the abdomen, which remained confined to the trunk. On the 7th day of hospitalization, she developed vesicles on the left retroauricular area, left upper eyelid, right axillary area, chest and abdomen. These vesicles gradually increased in size and number. On examination, she had pallor, bilateral cervical lymphadenopathy, multiple tense blisters over apparently normal skin, oral erosions over the hard palate, and redness of the left eye. Nikolsky′s sign was negative. The second patient was a 20-year-old female who presented with arthritis of both ankle and wrist joints with low grade fever, swollen feet and face and bullous lesions over the face and neck. She was a known case of nephrotic syndrome since the last 1 year and gave a history suggestive of photosensitivity. Examination revealed pallor, edema, and tense bullae over normal appearing skin of the face [Figure - 1] and lateral aspect of the neck. Nikolsky′s sign was negative and there were no oral lesions. Both the patients were subjected to hematological and biochemical investigations and histopathological study [Table - 1]. Direct immunofluorescence could not be done because this facility was not available. On the basis of the above findings, a diagnosis of bullous SLE was made. Both the patients were treated with dapsone 100 mg orally once daily. The maculopapular rash disappeared within 3 days of institution of therapy in the first patient, and the bullae started regressing by the 7th day. Ultimately, the lesions healed with residual hyperpigmentation. However, in the second patient, the bullous lesions did not respond till the 15th day and regressed very slowly thereafter, showing complete resolution with hyperpigmentation by the 45th day. Bullous systemic lupus erythematosus is a rare condition, with an incidence of 0.2 per million. It predominantly affects young adult females.[2] Tense bullae appear predominantly over the face, neck and upper trunk. Oral ulcerations, photosensitivity and glomerulonephritis may be associated. The target antigen is type VII collagen, but at times other antigens may be involved.[3],[4] Clinically similar, dermatitis herpetiformis and bullous pemphigoid can be differentiated by direct immunofluorescence. Bullous lesions in SLE due to photosensitivity, acute lupus or drugs can be differentiated by both histopathology and immunopathology. Epidermolysis bullosa acquisita (EBA) is histopathologically and immunopathologically identical since both diseases are mediated by circulating antibodies against type VII collagen. However, a dramatic therapeutic response to dapsone in bullous SLE differentiates it from EBA.[5] Both of our patients were young adult females having lesions predominantly in the head and neck region which is consistent with the reports of other authors.[1],[2], [6] Both had renal abnormalities and both of them responded to dapsone. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05019f1.jpg] [dv05019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}