 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
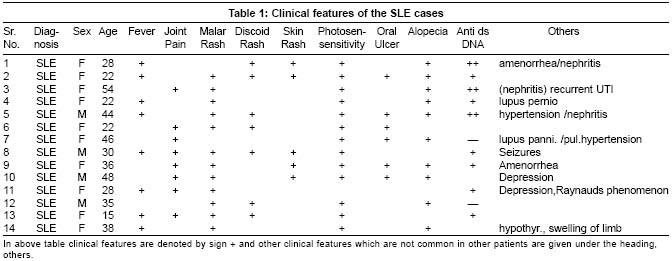
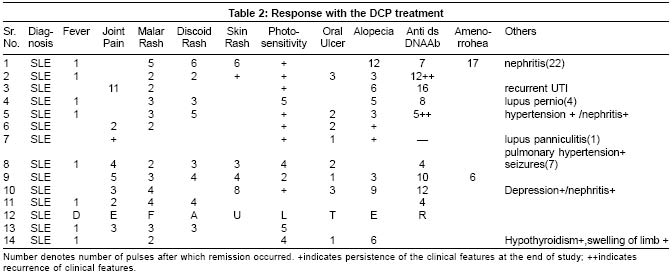
Indian Journal of Dermatology, Venereology, Leprology, Vol. 71, No. 1, January-February, 2005, pp. 9-13 Studies Dexamethasone-cyclophosphamide pulse therapy in systemic lupus erythematosus Dhabhai Ravindra, Kalla G, Singhi MK, Ghiya BC, Kachhawa Dilip Departments of Skin and V. D., Dr. S. N. Medical College, Jodhpur, Rajasthan Code Number: dv05024 ABSTRACT BACKGROUND AND AIMS: Therapy systemic lupus erythematosus (SLE) has been generally discouraging. Methyl-prednisolone pulse therapy has been used for various connective tissue disorders. We used intravenous dexamethasone cyclophosphamide pulse therapy to treat SLE.METHODS: Fourteen patients (10 females and 4 males) between the age of 15-48 years with definite or classical clinical criteria laid by American Rheumatism Association criteria were treated by Dexamethasone-Cyclophosphamide pulse (DCP) therapy at our center. RESULTS: It was possible to induce a complete clinical remission with DCP therapy in most of the patients thereby offering them life free from disease and drugs. The side effects commonly observed with conventional daily dose regimen of corticosteroids were not present or were mild. CONCLUSIONS: Almost all patients had good response after 3-4 pulses to allow them a normal life style. Fever, malar rash and oral ulceration responded early but photosensitivity, discoid rash, alopecia and joint pains took some more time. KEY WORDS: Systemic lupus erythematosus, Dexamethasone-cyclophosphamide pulse therapy, DCP therapy. INTRODUCTION Systemic lupus erythematosus (SLE) is a systemic disease characterized by the association of immunological abnormalities with pathological changes affecting a number of organ systems.[1] A range of auto-antibodies is found in SLE, although some of these are disease specific (anti-ds DNA and anti-Sm antibodies) and some are much more commonly found (anti-nuclear and anti-Ro antibodies).[2] Therapy in SLE has been generally discouraging. Methyl-prednisolone pulse therapy has been used for various connective tissue disorders and also in reversal of renal allograft rejection.[2],[3],[4],[5] Pasricha has reported success with pulse therapy in certain disorders like pemphigus, Reiter′s disease and pyoderma gangrenosum.[1] Previously Garg and Kalla[13] also treated some cases of SLE with dexamethasone-cyclophosphamide pulse (DCP) therapy at our center. We treated an additional 14 cases of SLE with the same regimen. METHODS This retrospective as well as prospective study was undertaken in the Department of Dermatology, Venereology and Leprology, Dr. Sampurnanand Medical College, Jodhpur and attached group of hospitals between November 1999 and May 2001. Fourteen patients (10 females and 4 males) between the age of 15-54 years satisfying the diagnostic criteria laid by American Rheumatism Association, were hospitalized. After taking detailed history and performing general and cutaneous examinations routine investigations such as complete hemogram, blood sugar, liver and renal function tests, serum electrolytes, urinalysis, stool examination for occult blood, semen analysis, ECG, chest x-ray were undertaken. Specific investigations like anti-dsDNA antibody (9 cases) were done in all whereas estimation of ANA was done in only two patients in whom anti-ds DNA was negative. Anti-Sm antibody, RA factor etc. were done in selected cases. Routine follow up to assess the response and complication of therapy was done with recording of blood pressure, history of epigastric pain, weight gain, striae atrophicans, hair loss, menstruation, urinary symptoms and eye examination for cataract. Relevant investigations were also performed during the follow-up period [Table - 1]. Before initiating the DCP therapy, a written informed consent of the patient was taken explaining the nature of disease, type of drugs to be administered with their possible side effects and outcome of the disease. Dexamethasone100 mg in 500 ml of 5% dextrose by slow intravenous infusion over a period of 1½ hour on 3 consecutive days once in a month was given together with 500 mg of cyclophosphamide added in the same intravenous infusion on any of the three days. Oral cyclophosphamide 50 mg daily was given between the courses of intermittent high dose therapy. In case no. 13 (who was unmarried) we gave only dexamethasone100 mg in 500 ml of 5% dextrose by slow intravenous infusion over a period of 1½ hour on 3 consecutive days once in a month. Patients were evaluated every 4th week according to clinical features recorded at the starting of the therapy. Pulse therapy was divided into four phases in which the first phase lasted up to remission of the disease process (clinical or laboratory), and the second phase was for a period of 6 months after disease remission. In the third phase only 50 mg oral cyclophosphamide was given for one year, and 2-3 year follow up was done without any treatment in the fourth phase. If disease process relapsed then the patient again entered the first phase of therapy. RESULTS There were 10 female and only 4 male patients. Surprisingly none of our female patients had onset of disease after menopause, the oldest patient was of 54 years and she had disease for the last 10-15 years, contrary to findings reported previously[6] where 15% of females had onset of their disease after menopause. While 14.2% of the patients had amenorrhea, another 14.2% suffered from irregular menstruation as a part of the disease process (polymenorrhea - 7.1%, menorrhagia 7.1%). Photosensitivity (13, 92.8%) was the most common clinical feature of SLE followed by malar rash (12, 71.4%), hair loss (10, 71.5%) and discoid rashes (7, 50%). Fever and joint pains were present in (8) 57.1%, oral ulcer/s in (6) 42.8%, nephritis in (3) 21.4%, and amenorrhea in (2) 14.2% patients. One female had chilblain lupus and another had subcutaneous tender nodules (lupus panniculitis) and pulmonary hypertension. Estimation of Anti ds DNA was done by Enzyme linked immunosorbent assay (ELISA) in 9 out of 14 cases. Quantification of this test varies according to manufacturer of the investigation kit. It was positive in 6 patients and negative in 3 cases. High cost factor didn′t allow us to go for Anti-ds DNA antibody estimation in all patients. Response was observed after the first pulse in almost all the patients. Seven out of 14 patients had complete clinical recovery and are being followed up. The average duration of follow up was 9 months, maximum duration of follow up being two years. Four patients are in phase II, as they are in remission and continuing the treatment while 3 are still receiving treatment (Phase I). Case 2 had a relapse during Phase III. Hence therapy was reinstituted and after 12 pulses she showed signs of clinical cure and is negative for anti-dsDNA. Fever was earliest to resolve in most of the cases after one pulse, oral ulceration cleared after 1-3 pulses. Malar rash showed remarkable improvement after 2-5 pulses in most cases but discoid rashes were difficult to treat as they took 2-16 pulses to resolve. Two females who had amenorrhea secondary to disease process started menstruating, one after 6 pulses (case 9) and another after17 (case 1). In one patient (case 7) who had lupus panniculitis, size of lesion and pain reduced up to 50% only after 1st pulse. She also had pulmonary hypertension as a concomitant finding; after 5 pulses she improved and was able to perform her regular domestic work without having exertional dyspnea. However, after a few months, during 8th pulse she died of cardiac arrest [Table - 2]. Patients with diffuse alopecia took 2-6 pulses for regaining a good growth of hair. Only one case took 17 pulses to regain cosmetically acceptable hair growth because to begin with she had complete loss of hair. Anti-ds DNA estimation showed good correlation with disease activity but not in all cases. It was positive in 6 patients and negative in 3 at the starting of treatment. Anti-ds DNA titer became negative/normal after 7 (case1), 12 (case2), 17 (case 3), 8(case 4) 15 (case 5) and 4 (case 10) pulses respectively. It again became positive in 2 cases (case 2 and 5). Case 2 was a female of 22 years, in whom titer became negative after 12 pulses and thereafter the patient was kept in Phase III but after one year it became positive again and therapy was reinstituted. This time it required 12 pulses to resolve. Similarly in case 5, titer came to normal after 15 pulses but after 5 months of Phase III it was again raised and the therapy was reinstituted and we required 10 repeat pulses to achieve normal level of titre. In 2 cases (case 11 and 13) t it remained positive after 4th pulse. Thereafter we couldn′t get their DsDNA titers due to unwillingness of these patients and in the rest of the cases it was not repeated due to the cost factor. The side effects usually associated with prolonged treatment of corticosteroids were virtually absent. Increase in weight, diabetes, hypertension, striae atrophicans, electrolyte imbalance, peptic ulcer, osteoporosis, cataract and hair loss were not seen. One of our patients was known hypertensive and he received the pulse treatment along with antihypertensive drugs without any complication. One patient had primary pulmonary hypertension and died of cardiac arrest. Bacterial and candidal infections of the skin and oral mucosa were the common side effects probably due to continuous immune suppression in almost all patients requiring frequent courses of antibiotics and systemic antifungals. Tuberculosis was reactivated in one patient during treatment that required antitubercular therapy. Pasricha et al[8] also observed such complications. Five patients had urinary tract infections (UTI), three of them having recurrent UTI, and were treated with appropriate antibiotics. Surprisingly, one patient used to develop fever a day after completion of three-day pulse schedule, whereas another developed urinary retention; they were managed appropriately. Menstrual irregularities were observed in 2 patients, one with polymenorrhea another with menorrhagia. In a study by McDermott et al[6] the incidence of premenopausal ovarian failure was 54% and the incidence of premature menopause (occurring before 40 year of age) 41% after treatment with cyclophosphamide pulse therapy. General darkening of complexion was noted in one patient with in one year of the treatment. Pasricha et al[7] reported similar pigmentation in 4 of their 79 pemphigus patients. Three patients (Case 4, 11 and 12) developed anemia after 5th, 10th and 5th pulse respectively requiring hematinics or blood transfusion. One patient developed pancytopenia, so pulse was withheld for 1 month and resumed again when counts became normal. Five patients complained of weakness / lethargy just after pulse therapy, in these patients short courses of small doses of oral corticosteroids were given. None of our patients had generalized pruritus and discomfort of the skin after DCP pulse therapy as observed by Pasricha et al.[8] None of the patients complained of hiccoughs, facial flushing, alopecia, stomach irritation and no one developed pancreatitis, cataract and seizures. We did not notice significant changes in laboratory parameters viz leukocytes count, blood glucose, electrolytes levels, platelet count and liver function tests. DISCUSSION Many studies have been done in India and abroad for the efficacy and safety of pulse therapy in various dermatological disorders like pemphigus vulgaris,[9],[10] systemic sclerosis,[11],[12] SLE,[13] infantile pyoderma gangrenosum,[14] and myositis.[15] Now it is being accepted as an established treatment modality. However, further studies and a long term follow up is required for the assessment of dexamethasone-cyclophosphamide pulse therapy to become the most preferred therapy for the various dermatological disorders that are difficult to treat with conventional modes of therapy. It was possible to induce a complete clinical remission with DCP therapy in most of our patients. The side effects commonly observed with conventional daily dose regimen of corticosteroids were not present or were mild in our patients. It reduced steroid induced obesity, striae atrophicans and chances of development of diabetes mellitus, osteoporosis, peptic ulceration, myopathy, cataract and hypertension. There are no absolute contraindications other than pregnancy and lactation. It is very essential to follow the treatment schedule to minimize the chances of relapse. By administrating supra-pharmacological doses of corticosteroids their immunosuppression activity was maximally used while minimizing the glucocorticoid activity. Almost all patients had good response after 3-4 pulses to allow them a near-normal life style. Fever, malar rash and oral ulceration responded early but photosensitivity, discoid rash, alopecia and joint pains took some more time. Anti-ds DNA estimation has strong correlation with the disease activity, hence in every case of SLE it should be estimated periodically if situation permits. The chief side effect observed was increased susceptibility to pyogenic and candidal infections of the skin and oral mucosa respectively, due to the immunosuppression induced by corticosteroids. This required frequent courses of systemic antibiotics and oral antifungals during initial months of therapy. The other side effects noted were menstrual irregularity (2), recurrent UTI (5), tuberculosis (1), dark complexion (1), hemorrhagic cystitis (3) rise in body temperature after every pulse (1), anemia (3), cardiac arrest (1). There was no correlation between the age of patient, and severity of involvement with effectiveness of DCP therapy. No significant adverse change in the laboratory parameters was seen in almost all cases. This treatment was safe in both diabetic as well as hypertensive patients. The duration of clinical activity after starting this regimen (phase I) had strong correlation with the time period between onsets of disease activity and initiation of therapy. Patients who reported early had a better response. It is necessary to follow up as long as possible in each of these patients for substantiation of the regimen. Patients should be educated well about severity of their disease and the compulsion to follow the treatment schedule strictly. Better cooperation on the part of the patient and supervision of the patient during therapy could minimize the chances of side effects and complications, thereby reducing both morbidity and mortality. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology, Leprology The following images related to this document are available:Photo images[dv05024t2.jpg] [dv05024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}