
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 71, Num. 5, 2005, pp. 316-320
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 5, September-October, 2005, pp. 316-320
Review Articles
Improving adherence to antiretroviral therapy
Nischal KC, Khopkar Uday, Saple DG*
Department of Dermatology and Venereology, Seth GS Medical College and KEM Hospital, Mumbai, *Department of Dermatology and
Venereology, Gokuldas Tejpal Hospital, Mumbai, India
Correspondence Address:Department of Dermatology and Venereology,
Seth GS Medical College and KEM Hospital, Parel, Mumbai-400 012, kc_nischal@yahoo.com
Code Number: dv05106
ABSTRACT
Antiretroviral therapy (ART) has transformed HIV infection into a treatable,
chronic condition. However, the need to continue treatment for decades
rather than years, calls for a long-term perspective of ART. Adherence
to the regimen is essential for successful treatment and sustained viral
control. Studies have indicated that at least 95% adherence to ART regimens
is optimal. It has been demonstrated that a 10% higher level of adherence
results in a 21% reduction in disease progression. The various factors
affecting success of ART are social aspects like motivation to begin therapy,
ability to adhere to therapy, lifestyle pattern, financial support, family
support, pros and cons of starting therapy and pharmacological aspects
like tolerability of the regimen, availability of the drugs. Also, the
regimen's pill burden, dosing frequency, food requirements, convenience,
toxicity and drug interaction profile compared with other regimens are
to be considered before starting ART. The lack of trust between clinician
and patient, active drug and alcohol use, active mental illness (e.g. depression),
lack of patient education and inability of patients to identify their medications,
lack of reliable access to primary medical care or medication are considered
to be predictors of inadequate adherence. Interventions at various levels,
viz. patient level, medication level, healthcare level and community level,
boost adherence and overall outcome of ART.
Keywords: Antiretroviral Therapy, Haart, Compliance, Adherence
INTRODUCTION
Antiretroviral drugs delay progression of HIV disease and improve the quality of life in the HIV infected. The "3 by 5" motto of WHO (treating 3 million by 2005) has provided impetus for greater use of antiretroviral therapy (ART) in developing and resource limited countries.[1] The advent of combination ART has transformed this disease into a chronic treatable condition for a significant proportion of people living with HIV and AIDS (PLWHA) with access to this treatment. However, the need to maintain patients on treatment for decades rather than years, calls for a long-term perspective of antiretroviral therapy.
A very high replication rate of HIV with increased susceptibility to
mutations in the process has led to the emergence of strains less sensitive
to antiretroviral agents.[2] The
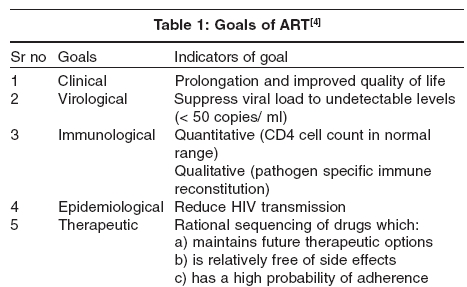
long lasting efficiency of ART starts with the initial decision to start
ART. The initial regimen plays an important role in achieving prolonged
viral suppression.[3] Therefore,
it must be chosen with the intent of achieving several goals [Table
- 1]. However, in cases with extensive prior drug exposure, the desired
goals are preservation of the immune system and prevention of clinical
progression rather than maximal viral suppression.[4]
With the availability of generic ART agents at a much lower cost, there
has been an increased use of ART in developing countries. Moreover, the
initial encouraging response seen with these drugs has prompted their
wide use across the medical fraternity, at times without considering
the serious consequences of mismanaged therapy. Hence it is prudent to
consider lack of adherence to ART, which adversely affects the overall
outcome.
Adherence to Therapy
Adherence to the regimen is essential for successful treatment and hence
has been rightly phrased as the ′Achilles heel of antiretroviral therapy′.[5] A major concern with ART is the emergence of viral resistance, which is mainly due to insufficient compliance. [4],[5],[6],
Other deterrents that hamper the outcome in ART are its lifelong duration,
serious side effects, the complexity of newer regimens, which may have
to be used due to the emergence of resistance, and the fact that therapy
is not curative. The adherence rate varies not just between individuals,
but also in the same individual over time,[7] thus
making adherence a variable rather than a stable characteristic of an
individual. Most people will exhibit low adherence at some time during
this extended therapy.[8] This
also makes the physician′s prediction of probable adherence achievable
by a patient highly unreliable.[9]
This makes it essential to define:
1. What is the optimal adherence required?
2. What are the implications of suboptimal adherence?
3. What are the factors to be considered to achieve optimal adherence?
4. What are the predictors of inadequate adherence?
5. What are the strategies to improve adherence?
What is the optimal adherence required?
Optimal adherence is the compliance to ART that achieves a sustained plasma drug concentration that will inhibit viral replication. Studies have indicated that at least 95% adherence to ART regimens is optimal. [6],[7],[8],[9],[10], With 95% adherence, viral suppression to below detectable levels occurs in 80%. However, a fall in adherence to 70% (i.e. 25% less than optimal) drastically decreases viral suppression to 33% (i.e. less than 50% achieved with optimal adherence).[10] Also, it has been demonstrated that a 10% higher level of adherence results in a 21% reduction in disease progression.[11] What are the implications of suboptimal adherence? A. Failure of the regimen
B. Increase in morbidity and mortality
C. Emergence of resistant strains of virus: If adherence is particularly poor, virologic failure is associated with a wild type of virus, but intermediate levels of adherence are likely to lead to the development of virus with resistant mutations in the genome.[12]
What are the factors to be considered to achieve optimal adherence?
Factors to be considered before starting ART are:
A. Social aspects
i. Motivation to begin therapy : Because of the long
course of therapy, the patient should be sufficiently motivated to begin
treatment.
ii. Ability to adhere to therapy : A busy work schedule may hinder
a patient from taking medications 6-hourly or 4-hourly, leading to poor
compliance.
iii. Lifestyle pattern : Extensive travelling,[13] substance
abuse and alcoholism[14] are
associated with poor adherence. The practice of meditation decreases
anxiety and strengthens mental resolve.[15] Spirituality
is an important dimension in the assessment of psychosocial factors affecting
HIV.[16],[17]
iv. Financial support : This is essential for this expensive
and prolonged treatment.
v. Family support : Expensive regimens and social stigma make
psychological and financial support by the family crucial.
vi. Pros and cons of starting therapy :[4] The
various pros and cons of starting therapy either early or late in the
course of disease must be considered and preferably discussed with the
patient.
B. Pharmacological aspects
i. Tolerability of the regimen : The drugs used in the regimen
have overlapping toxicities, which hamper adherence and cause organ dysfunction.
ii. Availability of drugs : Most of the newer and secondary regimen
drugs are not widely available.
Considerations should also be given to the regimen′s pill burden,
dosing frequency, food requirements, convenience, toxicity and drug interaction
profile compared with other regimens.
What are the predictors of inadequate adherence? Apart from the social and pharmacological aspects mentioned, there are some more factors that predict poor adherence:[4]
A. Poor interpersonal relation between the patient and the treating physician.
B. Active psychiatric illness (e.g. depression).
C. Inability of illiterate patients to identify medications.
D. Restricted access to primary medical care or medications.
What are the possible interventions to improve adherence?
Possible interventions that could be done at various levels to improve adherence are:
A. Interventions at the patient level
- Achieve a good rapport with the patient.
- Educate the patient about the disease and its course.
- Assess and establish the patient′s readiness to take medication.
- Discuss the goals of therapy, need for adherence, and the outcome
with the patient.
- Make him understand that the initial regimen has the best chance
for long-term success.
- Implement a treatment plan that the patient understands and to which
he/she commits.
- It is essential to discuss the importance of the impact of resistance
on future options andwhat to do if doses are missed, delayed,
or vomited. [4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],Daily
or weekly pillboxes, timers with alarm, pagers or other devices
can be used to remind patients of doses.
- Use visual aids and audio/video information sources for patients
with low literacy levels.
- Factors like sex, race, low socioeconomic status or education level
and past drug use are not reliable predictors of suboptimal adherence.[8]
-
Assessment of behavioral skills (goal-setting, time-tabling, assertiveness/communication,
problem-solving, etc.) and behavioral determinants of adherence
(daily routine, e.g. eating, sleeping and working patterns; recreational activities;
familial/social relationships and responsibilities; travel plans,
etc.)
are necessary for ensuring adequate adherence. [4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],
B. Interventions at the medication/ treatment level
- Implement a tailor made regimen for each patient after
thoughtful consideration of the simplicity or complexity of the regimen.
- Use the best of medications locally available.
- Consider the cost factor whenever and wherever applicable.
- Be aware of the job constraints, especially for a regimen requiring
doses to be taken 4- or 6-hourly. Keep the dose frequency and number of pills
to the minimum.
- Convey the common and probable side effects of ART to the patient
before starting therapy. This awareness improves the patient′s
confidence in the physician and hence the adherence. Anticipate side
effects and treat them as soon as possible.
- Modify the dietary pattern to suit the antiretroviral agents.
- Avoid adverse drug interactions amongst ART drugs and drugs used
for controlling other symptoms as well as opportunistic infections.
- Detect and treat any intervening illness and opportunistic infections
at the earliest.
- Direct observed therapy (DOTS) and modified DOTS are being explored
to enhance adherence.[19],[20] Their
relevance in resource limited countries is speculative at present.
C. Interventions at the healthcare delivery level
It is essential to establish a health care team comprising
of clinicians, psychologists and volunteers to cater to the various
needs
of HIV patients.
It is but natural to expect a reduction in adherence as time progresses,
even among patients whose adherence has been optimal. This phenomenon
is termed as ′pill fatigue or treatment fatigue,[21],[22] Regular
and intensive monitoring is the only solution to this. Though there
are many methods to measure adherence to ART like electronic, pill
count,
drug assay, MEMS cap (medication event monitoring system), provider
estimates and visual analogue scale,[23] in
clinical practice, the most efficient method is to simply ask the patient
in supportive and non-judgmental ways. Most patients are truthful about
their medication taking when asked.[24]
To get the most reliable information, the patient should be given the
chance to err with dosages and should be asked in a non-judgmental
way and given a specific period. For example, "Everyone misses doses
some of the time. In the last two weeks, how many doses have you missed?"[25] This
self-reporting technique of adherence measurement makes patients aware
of the importance of their role in the achievement of optimal adherence.
Other measures to improve adherence include:
- Serve as an educator and an information source with ongoing
support and monitoring. Adherence to antiretroviral therapy is improved
where patients view their relationship with their doctor positively.[26]
- Supportive and non-judgmental attitudes and behaviours encourage
the patient′s
honesty regarding adherence and associated problems.
- Provide access between visits for any problems or queries, including
during vacations (e.g. by providing pager number etc.).
- Intercurrent medical, surgical or psychological illness (e.g. liver
disease, wasting, recurrent chemical dependency) can adversely affect adherence
and necessary modification in management is essential
- Offer specific training to all health care team members and periodically
update them.
Alternative medicines are in common use by patients with chronic
ailments and this is true with HIV infected patients too. Traditional
healers
still play a major role in providing initial health care in
many developing countries and the possibility of involving them in
the HIV health care
system for better patient care is being explored.[27],[28]
D. Interventions at the community level
The apprehension of social ostracization is a major hindrance to adherence as it limits a patient from taking medications in front of others, especially with complex regimens. Thus, the psychological support by the family and friends is a major factor in antiretroviral therapy.
- Recruit family and friends to support the treatment plan.
- Develop a link with local community based organizations regarding
adherence combined with educational sessions and practical strategies.
- Use peer education for adolescents and injection drug users.
- Encourage HIV affected patients to form support groups, which guide
and help others in coping up with the situation.
- Mobilize sufficient funds for expensive medications through charitable
trusts and NGOs.
- Vocational and occupational rehabilitation.
In India, there is complete lack of awareness among the masses regarding
ART. Health care providers need vigorous training in delivering all aspects
of ART.
Busy medical practitioners find it difficult to spare enough time for the
extended counseling that is needed for the success of any therapy, especially
ART. Moreover,
adequate supply of medicines for ART as well as for treating opportunistic
infections is essential for achieving the expected adherence to ART.
REFERENCES
| 1. | Scaling up antiretroviral therapy in resource limited settings: Treatment guidelines for a public health approach. 2003 revision. World Health Organization, Geneva, 2004. http://www.who.int/hiv/pub/prev_care/en/arvrevision2003en.pdf Last accessed on 14.04.2005. Back to cited text no. 1 |
| 2. | Gazzard BG. Factors to consider when introducing antiretroviral treatment. J HIV Ther 2002;7:3-6. Back to cited text no. 2 [PUBMED] |
| 3. | Bini T, Testa L, Chiesa E, Adorni F, Abeli C, Castelnuovo B, et al . Outcome of second-line protease inhibitor-containing regimen in patients failing or intolerant of a first highly active antiretroviral therapy. J AIDS 2000;24:115-22. Back to cited text no. 3 |
| 4. | Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents. Panel on clinical practices for treatment of HIV Infection convened by the Department of Health and Human Services (DHHS), USA. Created on October 29, 2004. http://aidsinfo.nih.gov/guidelines/adult/AH_102904.pdf. Last accessed on 14.04.2005. Back to cited text no. 4 |
| 5. | Sherr L. Understanding adherence. J HIV Ther 2000;5:30-5. Back to cited text no. 5 |
| 6. | Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN, Squier C, et al . Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med 2000;133:21-30. Back to cited text no. 6 |
| 7. | Carrieri P, Cailleton V, Le Moing V, Spire B, Dellamonica P, Bouvet E, et al . The dynamic of adherence to highly active antiretroviral therapy: results from the French National APROCO cohort. J Acquir Immune Defic Syndr 2001;28:232-9. Back to cited text no. 7 |
| 8. | Horne R. Adherence to medication: a review of existing research. In: Myers L, Midence K, editors. Adherence to treatment in medical conditions, 1st edn. London: Harwood Academic; 1998. p. 285-310. Back to cited text no. 8 |
| 9. | Crespo-Fierro M. Compliance/adherence and care management in HIV disease. J Assoc Nurses AIDS Care 1997;8:43-54. Back to cited text no. 9 |
| 10. | Arnsten JH, Demas P, Gourevitch M, Buono D, Farzadegan H, Schoenbaum E. Adherence and viral load in HIV-infected drug users: comparison of self-report and medication event monitors (MEMS). Program and Abstracts of the 7th Conference on Retroviruses and Opportunistic Infections; January 30-February 2, 2000; San Francisco CA. Abstract 69 (poster). Back to cited text no. 10 |
| 11. | Bangsberg DR, Perry S, Charlebois ED, Clark RA, Roberston M, Zolopa AR, et al . Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS 2001;15:1181-3. Back to cited text no. 11 |
| 12. | Walsh JC, Pozniak AL, Nelson MR, Mandalia S, Gazzard BG. Virologic rebound on HAART in the context of low treatment adherence is associated with a low prevalence of antiretroviral drug resistance. J Acquir Immune Defic Syndr 2002;30:278-87. Back to cited text no. 12 [PUBMED] [FULLTEXT] |
| 13. | Salit IE, Sano M, Boggild AK, Kain KC. Travel patterns and risk behaviour of HIV-positive people travelling internationally. CMAJ 2005;172:884-8. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Samet JH, Horton NJ, Meli S, Freedberg KA, Palepu A. Alcohol consumption and antiretroviral adherence among HIV-infected persons with alcohol problems. Alcohol Clin Exp Res 2004;28:572-7. Back to cited text no. 14 [PUBMED] [FULLTEXT] |
| 15. | Telles S, Naveen KV. Yoga for rehabilitation: an overview. Indian J Med Sci 1997;51:123-7. Back to cited text no. 15 |
| 16. | Avants SK, Warburton LA, Margolin A. Spiritual and religious support in recovery from addiction among HIV-positive injection drug users. J Psychoactive Drugs 2001;33:39-45. Back to cited text no. 16 [PUBMED] |
| 17. | Tuck I, McCain NL, Elswick RK Jr. Spirituality and psychosocial factors in persons living with HIV. J Adv Nurs 2001;33:776-83. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | British HIV Association (BHIVA) / British Association for Sexual Health & HIV (BASHH) guidelines on provision of adherence support to individuals receiving antiretroviral therapy. Poppa A, Davidson O, Deutsch J, Godfrey D, Fisher M, Head S, Horne R, Sherr L. Created in 2003. http://www.bhiva.org/guidelines/2004/adherence/index.html Last accessed on 14.04.2005. Back to cited text no. 18 |
| 19. | Mitty JA, Stone VE, Sands M, Macalino G, Flanigan T. Directly observed therapy for the treatment of people with HIV infection: A work in progress. Clin Infect Dis 2002;34:984-90. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Kagay CR, Porco TC, Liechty CA, Charlebois E, Clark R, Guzman D, et al. Modeling the impact of modified directly observed antiretroviral therapy on HIV suppression and resistance, disease progression, and death. Clin Infect Dis 2004;38:S414-20. Back to cited text no. 20 [PUBMED] [FULLTEXT] |
| 21. | Mannerheimer S, Friedland G, Matts J, Chen L, Child C, MacArthur R, et al . Self-reported antiretroviral adherence correlates with HIV viral load and declines over time. 13th International AIDS Conference. Durban: South Africa 2000 . Abstract No. Tu Or B 421. Back to cited text no. 21 |
| 22. | Nieuwkerk P, Burger D, Hugen P, Aarnoutse R, Van Heeswijk R, Veldkamp A, et al . Patient adherence to highly active antiretroviral therapy for HIV-1 infection in a nationwide cohort study in the Netherlands. 13th International AIDS Conference. Durban: South Africa 2000 . Abstract No. Mo Pp D 1055. Back to cited text no. 22 |
| 23. | Giordano TP, Guzman D, Clark R, Charlebois ED, Bangsberg DR. Measuring adherence to antiretroviral therapy in a diverse population using a visual analogue scale. HIV Clin Trials 2004;5:74-9. Back to cited text no. 23 [PUBMED] [FULLTEXT] |
| 24. | Sackett DL, Haynes RB, Gibson ES, Hackett BC, Taylor DW, Roberts RS, et al . Randomized clinical trial of strategies for improving medication compliance in primary hypertension. Lancet 1975;1:1205-7. Back to cited text no. 24 |
| 25. | Cheever LW. Adherence to HIV therapies. In: Jean R Anderson, editor. A guide to the clinical care of women with HIV, Maryland: Department of Health and Human Services (DHHS), USA; 2001. p. 139-48. Back to cited text no. 25 |
| 26. | Altice FL, Mostashari F, Friedland GH. Trust and the acceptance of and adherence to antiretroviral therapy. J Acquir Immune Defic Syndr 2001;28:47-58. Back to cited text no. 26 [PUBMED] [FULLTEXT] |
| 27. | Homsy J, King R, Tenywa J, Kyeyune P, Opio A, Balaba D. Defining minimum standards of practice for incorporating African traditional medicine into HIV/AIDS prevention, care, and support: a regional initiative in eastern and southern Africa. J Altern Complement Med 2004;10:905-10. Back to cited text no. 27 [PUBMED] [FULLTEXT] |
| 28. | Homsy J, King R, Balaba D, Kabatesi D. Traditional health practitioners are key to scaling up comprehensive care for HIV/AIDS in sub-Saharan Africa. AIDS 2004;18:1723-5. Back to cited text no. 28 [PUBMED] [FULLTEXT] |
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv05106t1.jpg]
|

{kind=link}