 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
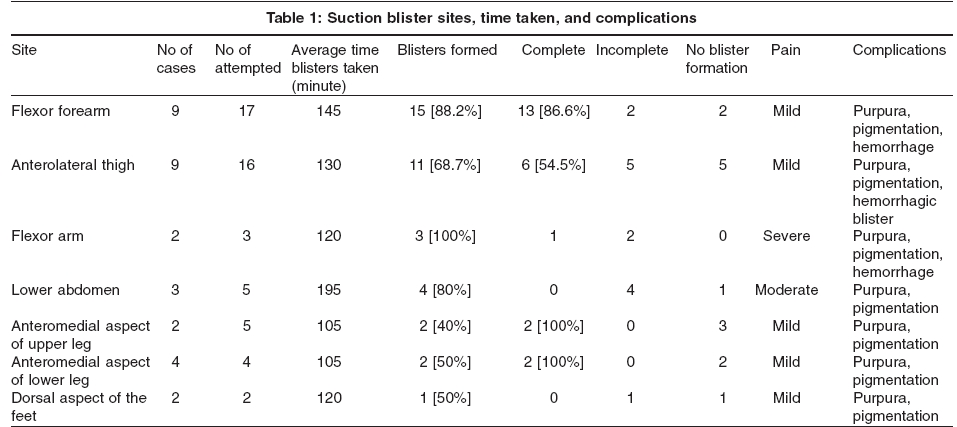
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 5, September-October, 2005, pp. 321-324 Studies Reliable site for suction blister induction and harvesting Laxmisha Chandrashekar, Thappa DevinderMohan Department of Dermatology and Sexually Transmitted Diseases, Jawaharlal Institute of Medical Education and Research (JIPMER), Pondicherry Code Number: dv05107 ABSTRACT Background: Suction blister grafting is a useful modality of treatment of patients with resistant and stable vitiligo. However, there have been no detailed studies to find out the best donor site for blister formation.Methods: The study was conducted between the period of October 2004 and February 2005 in the dermatology department at a tertiary care center. Nine patients with vitiligo (focal vitiligo, 3; mucosal vitiligo, 2; acrofacial vitiligo, 2; vitiligo vulgaris, 1; and segmental vitiligo, 1) were selected for blister harvesting and grafting. The blisters were raised using the method described by Gupta et al. Results: Suction blisters were attempted to be raised at 52 sites, but only 38 blisters could be raised, 24 complete and 14 incomplete. Blisters were raised in all the three cases on the flexor aspect of the arm (100%), 15 of 17 cases (88.2%) on the flexor aspect of the forearm, 4 of 5 cases (80%) on the abdomen, 11 of 16 cases (68.7%) on the anterolateral thigh, and less frequently over leg or foot. Complete blisters were formed in 13/15 cases (86.6%) on the flexor aspect of the forearm, 6/11 cases (54.5%) on the anterolateral thigh, and in all cases over leg. Conclusion: The flexor aspect of the forearm is a good site for suction blister harvesting. Keywords: Suction Blister, Donor Site INTRODUCTION Suction blister grafting is a useful modality for the treatment of patients with resistant and stable vitiligo.[1] Numerous alternatives have been used to produce a blister, such as double-syringe devices connected to a three-way connector, a combination of syringes and a cylinder funnel, an angiosterometer, and a modified conventional gastric or respiratory suction pump.[2] However, there have been no detailed studies to find out the best donor site for blister formation. This study aimed to find the best and most reliable site for blister harvesting. METHODS The study was conducted between the period of October 2004 and February 2005 in the dermatology department at a tertiary care center. Patients with stable vitiligo for more than one year were recruited. All of them had been on treatment with superpotent or potent topical corticosteroids, oral minipulses with oral corticosteroids, topical PUVA therapy or topical tacrolimus for at least 6 months. None of them had any keloidal or bleeding tendencies. Patients with coexistent herpes simplex infections were excluded from the study. All patients were counseled prior to the procedure regarding the risks, benefits and anticipated outcome. All patients were given an analgesic prior to the procedure. The blisters were raised using the method described by Gupta et al.[1] Sites over joints and uneven areas (which hinder the application of a syringe for suction), or with hairy and tight recipient skin (which impedes blister formation) were not selected for blister induction. More blisters were raised compared to recipient area as complete blister formation was not assured in each patient. The device used for inducing a blister consisted of 20 and 50 ml syringes, three-way taps, a pressure gauge and latex rubber tubes. Twenty ml disposable syringes were used as suction cups. Their needle ends were attached to three-way taps with small rubber tubes. Suction was attempted by means of a 50 ml syringe attached to the opposite end of the three-way tap. Vacuum was retained, by locking the suction-syringe end of the three-way tap. Once the desired pressure of -300 mm Hg was attained, the suction syringe end was locked. The patient′s pain was assessed on a subjective- mild, moderate and severe scale. A complete blister was defined as a solitary hemispherical unilocular bulla with a diameter of 3 cm, and an incomplete blister as one in which there were multiple small vesicles or a partial bulla with a diameter of less than 3 cm. The results were analyzed using the following parameters: number of cases with complete or incomplete blister formation, time taken for blister formation, and rate of complications. The results were analyzed using chi square test. RESULTS Nine patients, seven males and two females, with vitiligo (focal vitiligo, 3; mucosal vitiligo, 2; acrofacial vitiligo, 2; vitiligo vulgaris, 1; and segmental vitiligo, 1) were selected for blister harvesting and grafting. Their average age was 24.2 years (range, 8 years to 43 years), and the average duration of vitiligo was 3.55 years (range, 1 year to 10 years). Blisters were raised on the flexor aspect of the forearm in 9 cases, anterolateral thigh in 9 cases, anteromedial aspect of the lower leg above the medial malleolus in four cases, lower abdomen in three cases, dorsum of the foot in 2 cases, anteromedial aspect of the upper leg in 2 cases, and flexor aspect of the arm in 2 cases. We attempted to raise 52 suction blisters at various sites [Table - 1], but only 38 blisters could be raised, 24 complete and 14 incomplete. No complete blisters were formed on the dorsum of the foot and over the abdomen. The average time taken for blister formation was 195 minutes for the lower abdomen, 145 minutes for the flexor aspect of the forearm, 130 minutes for the anterolateral thigh, 120 minutes for the dorsum of the foot and flexor aspect of the arm, and 105 minutes each for the anteromedial aspect of the upper leg and the anteromedial aspect of the lower leg above the medial malleolus.
Immediate complications included purpura at the margin of application of the suction syringe (52 cases) and pigmentation at the donor site (52 cases), which started as early as one week after the procedure. This pigmentation lasted for as long as two months before it started subsiding. By the end of 3 months, an imperceptible macular pigmentation remained in most of the cases (51 of 52 cases); there was marked pigmentation in one case where the blister was raised on the forearm. We did not attempt to raise blisters at all sites. The anteromedial aspect of the leg was not selected due to the possibility of delayed wound healing. Only a limited number of blisters could be raised on the dorsum of the foot, anteromedial aspect of the upper leg, and anteromedial aspect of the lower leg above the medial malleolus. Hence, these sites were not used further. Due to the severe pain and limited area, the flexor aspect of the arm was abandoned as a site for raising blisters. Incomplete blisters and pain precluded the abdomen as a site for blister grafting. Multiple blisters could be raised on both the flexor aspect of the forearm and the anterolateral thigh with mild pain. On comparison of the nature of blister formation at these two sites, complete blisters were significantly associated with those raised over the flexor aspect of forearm as compared to the anterolateral thigh (p < 0.05). There was no significant difference (p > 0.05) between the results in males and females. DISCUSSION Surgical methods for harvesting normally pigmented donor skin include Thiersch′s grafts,[3] split thickness skin grafts[4] and mini-punch grafts.[5] They have been practiced for many years with good results but have not gained wide popularity as they require anesthesia. In addition, the surgery carries a risk of damage to the dermis and hence scarring. In contrast, autologous epidermal transplantation (AET) using the roofs of suction blisters is an effective, non-scarring, surgical repigmentation method that has become popular since 1971, when Falabella first described its use in leukoderma. [6],[7],[8],[9], The results are most remarkable with segmental vitiligo, especially on the face.[10] Falabella induced blisters by using a negative pressure of approximately 300 to 500 mm of Hg on the donor sites.[6] Rusfianti and Wirohadidjodjo used a 20-ml syringe connected to a respiratory suction pump over the lower abdominal skin to induce blisters. Blister induction took approximately 2 hours.[2] Blister formation is difficult and more time consuming when the patients are young.[2] Blistering occurs due to destruction of desmosomes along the basement membrane. The weak dermoepidermal adherence in the elderly makes the separation easier and faster. Some techniques can reduce the time required for blister formation, such as intradermal injection of normal saline, application of heat, increase of negative pressure by 100 mm Hg when small vesicles appear, and selecting donor skin that overlies the greater trochanter. Koga found that the abdomen and the thighs are the most suitable donor areas.[11] However, even then blister formation takes approximately 4 to 5 hours. Gupta et al observed that the anterolateral thigh requires the least time (1.5 hours) for formation of a blister and postulated that this was due to the close proximity of the skin to the bone making the skin tense.[1] The suction blister induction time (SBIT) is directly proportional to the diameter of the suction syringe.[12] The site of the suction blister, the subject′s age, amount of vacuum created, temperature, intradermal injection of saline, corticosteroid-induced atrophy, and pretreatment of the site with PUVA are the important factors that influence the SBIT.[12] Use of 10 ml or 20 ml syringes as suction cups and -300 mm Hg pressure are appropriate choices for suction blister induction. They usually produce blisters in about 1-2 hours. We found that the flexor aspect of the forearm is probably a better site for raising suction blisters (blisters were raised in 88.2% of blister sites over this site compared to 68.7% of blister sites over the anterolateral thigh). Complete blisters were formed in 13 of 17 blister sites over the flexor aspect of the forearm compared to 6 of 16 blister sites over the anterolateral thigh. This was statistically significant (p < 0.05). Chances of blister formation were highest over the flexor aspect of the forearm. The reason for this could be the presence of underlying muscles and tendons. There was no significant difference in the SBIT over the flexor aspect of the forearm and the anterolateral thigh (145 vs. 130 minutes). We conclude that the flexor aspect of forearm is a good site for suction blister harvesting as it is easily accessible, the patient is more comfortable, and blister induction is likely to be more successful. However, if more grafts are needed, the anterolateral thigh can be used. Our study had some limitations like a small sample size, not choosing the bikini area in females, not comparing non-hairy areas with hairy areas, and not choosing the medial aspect of the forearm (probably the best donor site next to the flexor aspect of the forearm). We could have also achieved better pain control by utilizing ice packs and topical EMLA. These parameters may be studied in better-designed studies. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05107t1.jpg] |
| |||||||||

{kind=link}