 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
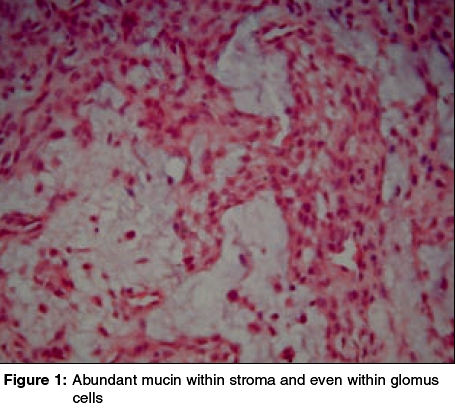
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 5, September-October, 2005, pp. 367-368 Letter To Editor Glomus tumor with mucinous change Godse KiranV Shree Skin Centre, 22, L Market, Sector 8, Nerul, Navi Mumbai - 400 706 Code Number: dv05124 Sir, Glomus tumors are relatively uncommon neoplasms arising from modified smooth muscle cells that are normally found in specialized arteriovenous shunts in acral sites, especially the fingertips. This distribution reflects their function because the arteriovenous anastomoses of these areas, also known as the Sucquet-Hoyer canals, are involved in temperature regulation. Sucquet-Hoyer canals are lined by endothelial cells, have several layers of glomus cells in their walls, and connect an afferent arteriole to an efferent venule.[1] A 30-year-old housewife presented with the complaint of a painful right index finger since one year. She used to get intense pain with slight trauma on touch. The right index finger nail was removed, but there was little relief from the pain. On examination, a small 8-10 mm sized bluish tender swelling was noted just below the right index fingernail. An excision biopsy of this lesion revealed a neoplasm composed of a reticular network of tumor islands made up of monomorphous rounded cells [Figure - 1]. The cells had abundant pink or pale blue cytoplasm and monomorphous oval nuclei. Several dilated thick walled vascular channels were also seen within these tumor islands. The stroma had abundant mucin, which appeared to be present within the neoplastic cells as well. Alcian blue stain confirmed the presence of abundant mucin within the stroma and the cells. Mucin in glomangioma is rarely reported. Hisa et al reported four cases with mucinous degeneration, the extent of which correlated with the number of glomus cells.[2] Glomus tumors are thought to originate from their normal counterpart (e.g. the glomus cells); therefore they tend to occur most commonly in acral areas.[3] The term glomus tumor is used to characterize two phenotypically different types of tumors: cutaneous glomangioma and paraganglioma. Both tumors can occur in a familial setting with an autosomal dominant pattern of inheritance.[5],[6] However, they are of different histopathologic origin. Paragangliomas derive from the APUD cell system, whereas cutaneous glomangiomas originate from glomus bodies of the skin, which are important in the regulation of body temperature.[7] An autosomal dominant pattern of inheritance has been described for glomus tumors of the paraganglioma type originating from the APUD cell system, the underlying genetic defect of which has been mapped to chromosome 11q23. In contrast, Blume-Peytavi et al showed that the genetic defect in disseminated cutaneous glomus tumors of the glomangioma type deriving from smooth muscle cells or pericytes is not linked to chromosome 11.[7] Thus, they suggested that the common term glomus tumor, used for both paragangliomas and glomangiomas in the current literature, is misleading and should be avoided because these tumors have different histologic derivations and genetic origins. REFERENCES
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05124f1.jpg] |
| |||||||||

{kind=link}