 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
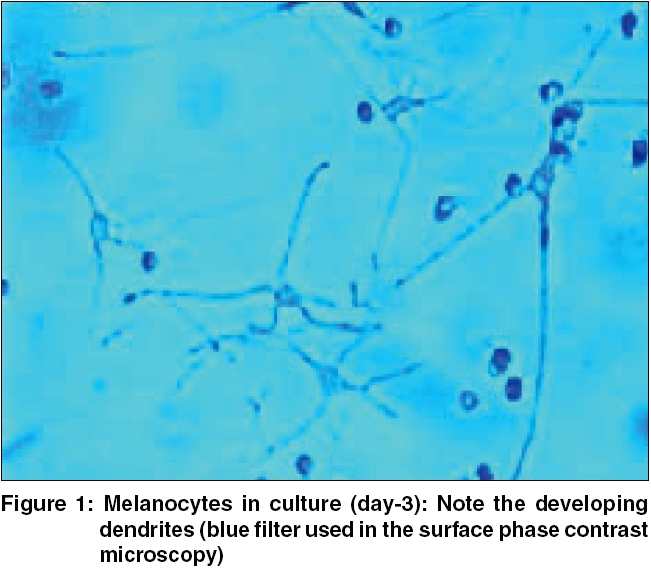
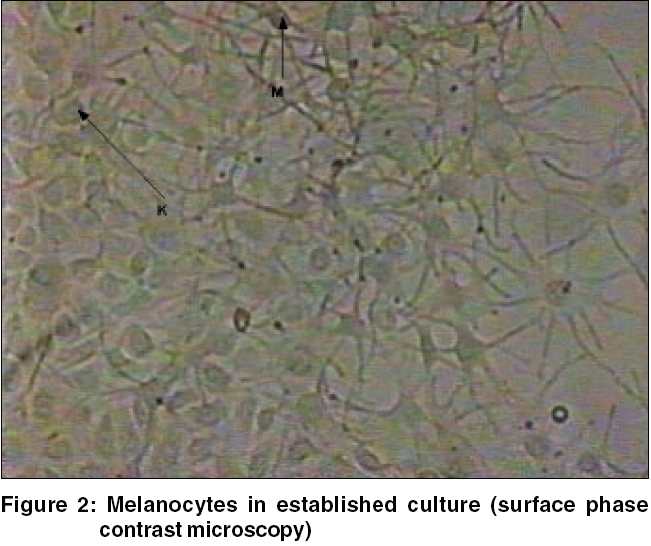
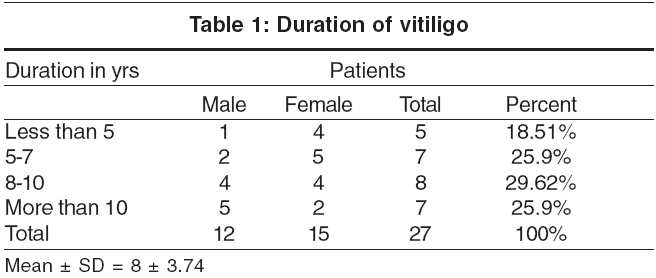
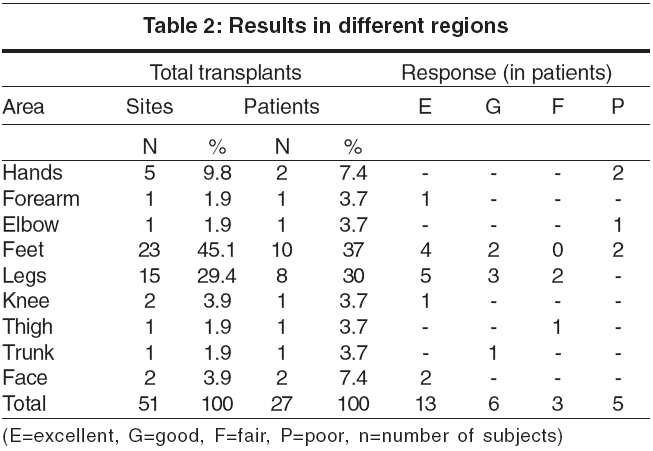
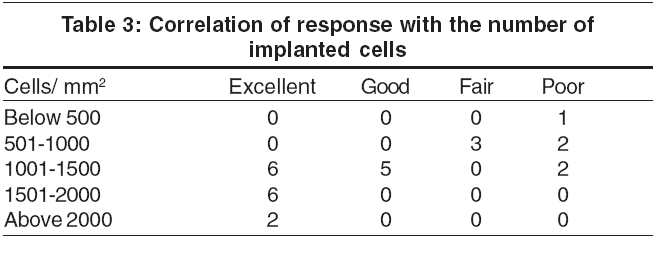
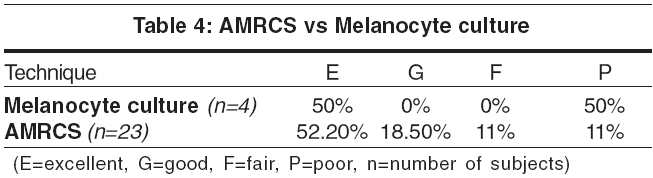
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 6, November-December, 2005, pp. 393-397 Original Article A study of autologous melanocyte transfer in treatment of stable vitiligo Pandya Vishvabhavan, Parmar KirtiS, Shah BelaJ, Bilimoria FE Department of Dermatology, Civil Hospital and BJ Medical College, Ahmedabad Code Number: dv05131 Abstract Background: Replenishing melanocytes selectively in vitiliginous macules by autologous melanocytes is a promising treatment. With expertise in culturing melanocytes, it has now become possible to treat larger recipient areas with smaller skin samples.Aim: To study the extent of repigmentation after autologous melanocyte transplantation in patients with stable vitiligo. Methods: The melanocytes were harvested as an autologous melanocyte rich cell suspension from a donor split thickness graft. Melanocyte culture was performed in selected cases where the melanocyte cell count was insufficient to meet the requirement of the recipient area. These cells were then transplanted to the recipient area that had been superficially dermabraded. Results: An excellent response was seen in 52.17% cases with the autologous melanocyte rich cell suspension (AMRCS) technique and in 50% with the melanocyte culture (MC) technique. Conclusion: Autologous melanocyte transplantation can be an effective form of surgical treatment in stable but recalcitrant lesions of vitiligo. Keywords: Autologous melanocyte transplantation, Melanocyte culture, Melanocyte rich cell suspension Introduction There are many modalities for the treatment of vitiligo but there is still a need for a treatment that is promptly effective. Replenishing melanocytes selectively within vitiliginous macules by autologous melanocytes is a promising treatment.[1] Moreover, with expertise in culturing melanocytes, it has now become possible to treat larger recipient areas with smaller skin samples.[1] There are a few techniques for seeding autologous melanocytes. To study the extent of repigmentation after autologous melanocyte transplantation in patients with stable vitiligo, we employed two methods, melanocyte rich cell suspension and cultured melanocytes for replenishing melanocytes.Methods Patients with stable vitiligo were selected for the study, the criteria for stability being no increase in the size of the lesion for at least 2 years and no new lesions since the last 2 years. Exclusion criteria were patients with active disease, infection at the recipient site, age below 8 yrs, evidence of Koebner response in the past, bleeding diathesis, keloidal tendencies and poor general condition. The study was conducted at Department of Dermatology, Civil Hospital, BJ Medical College, Ahmedabad in a span of 3 years. Patients were chosen randomly after they met the selection criteria. Out of the 27 patients recruited, a single vitiliginous lesion was taken as a control in 20 cases. The control patch was only superficially dermabraded and subsequently dressed. Pre-operative work-up consisted of informed consent, a clinical photograph, screening for HIV and Hepatitis B virus infection and charting of the area to be grafted. A prophylactic course of an antibiotic, usually oral erythromycin 500 mg thrice daily, was started 1 day before the procedure and alprazolam 0.5 mg was administered orally on the previous night. Two techniques were employed, the autologous melanocyte rich cell suspension (non-cultured) technique[1],[2],[3] and the cultured melanocyte technique. [4],[5],[6] Both these techniques share a common principle of selective replenishment of melanocytes at the recipient stable vitiligo macules. The culture technique was used when the harvested melanocytes were less than required, when counted with Neubauer′s chamber. Donor site Laboratory procedure for cell separation[3] Recipient site Transplantation[1] The patient was allowed to go home 30 minutes later. The dressing was removed at their first follow-up visit after a week to the hospital. Preparation of autologous culture of melanocytes[4] Erythromycin and nimesulide 100 mg daily (if required) were continued for 7 days following the transplantation. The dressings at the donor and recipient site were removed on day 7. A light dressing was applied on the recipient area for the next 7 days, if found necessary. The patient was called after 1 month, 3 months and 6 months to assess the extent of repigmentation. Photographs were taken and the observations were tabulated. The response was graded according to the extent of repigmentation in transplanted areas as follows: excellent, >90% repigmentation; good, 65% to 89% repigmentation; fair, 25% to 64% repigmentation and poor, below 25% repigmentation. Results Of the total 27 patients with vitiligo, 12 (44.45%) patients were male and 15 (55.55%) female. Majority (16, 59%) of the patients were in the age group of 21 to 30 years. Vitiligo was of the vulgaris type in 25 and segmental type in 2 patients. [Table - 1] shows details of duration of disease in our patients. At first follow-up, soon after the removal of dressing the treated area appeared bright pink. Repigmentation was first seen after 2-3 weeks after the procedure and was completed in up to 6 months. It was almost of a uniform color. In a few cases, there was initial hyperpigmentation that subsequently faded to match the normal skin color.[1] This hyperpigmentation may be caused by hyperactivity of transplanted cells from the culture or oversupply of growth factors and melanogenic peptides such as β-FGF during wound healing.[1],[7] In most patients we observed pigmentary islands irrespective of leukotrichia or paucity of hair follicles. The optimum time for successful culture was 1-3 weeks. At the end of 3 weeks, the cell count was raised 50-100 folds after primary culture and subculture. The melanocyte content of these cultures was 95%. Fifty-one sites in 27 patients were chosen for autologous melanocyte transplantation. The most common sites were the feet (45.1%), legs (29.4%), hands (9.8%), knees (3.9%) and face (3.9%) [Table - 2]. The results were most favorable on the legs, feet, face and forearms, and poor on the elbows and acral areas of the hand. Repigmentation was not observed in any of the control patches. The repigmentation was best when there were 1500 cells/mm2 or more. In 27 patients, the cells were cultured because of the large recipient area or because the number of cells separated was less than 1000 cells/sq cm of recipient area [Table - 3]. An excellent response was seen in 12 (52.2%) and 2 (50.0%) patients with AMRCS and melanocyte culture respectively [Table - 4]. Some minor complications were observed. Strikingly, there was no milia formation or scarring. Two (7.4%) patients had infection at the donor area and three (11.1%) developed infection at the recipient surface. Only one patient developed K φebner response at the donor area. Discussion Both, the autologous melanocyte rich cell suspension (non-cultured) technique and the cultured melanocyte technique, are essentially based on the principle of seeding of melanocytes. Melanocyte culture is a state of the art procedure that requires expertise. Superficial split thickness thin skin grafts (STG) yielded more melanocytes than did punch biopsy samples chiefly because of the larger size of skin harvested and because separation of cells was easier with thinner samples of skin. Moreover, the STG donor sites healed better. The average number of cells kept was 1000-1500 cells/mm2 irrespective of the technique employed. The outcome was optimal when more than 1000 cells form AMRCS/mm2 were kept but was proportionately less when the number was less. The autologous melanocyte rich cell suspension (AMRCS) technique of autologous melanocyte transfer was equally effective for smaller lesions but for a larger recipient area, melanocyte culture (MC) was found more suitable, although the technique of AMRCS was simple and efficient.[11] Overall, an excellent response was seen in 14 patients (51.8%), a good response in 5 (18.5%), and a fair response in 3 (11.1%). Five patients (18.5%) had a poor response. Response to both techniques was comparable, with an excellent response in 52.2% cases of the AMRCS technique and 50% with melanocyte culture. Repigmentation was generally first observed at 2-3 weeks and was complete by 6 months. It was seen as multiple islands of pigmentation that later coalesced to a uniform color. The location of the recipient site was the major determinant of the outcome; acral parts including the dorsal aspects of the hands and feet, and skin over the joints were less responsive, as 2 patients each with lesions on the hands and feet, and 1 patient with lesions on the elbow had a poor response.[1] The response was comparable to studies done by Mulekar.[9] In a study in 27 patients, Lontz et al reported excellent response in 40.7%, good response in 7.4%, and moderate response in 51.8%.[1] Lontz et al emphasize that the anatomical location is the major factor that determines the response.[1] The fingers, knuckles and elbows were the most difficult areas to repigment, in part because of the relative uncertainty in controlling the depth of dermabrasion of such heavily cornified areas and also because of the high mobility of the skin covering these joints. Olsson and Juhlin have also made a similar observation.[4] Both these techniques had some minor complications. Infection at the donor area was seen in 7.4% of patients and at the recipient site in 11.1%. Infection occurred probably because patients did not comply with instructions to avoid unnecessary movements of the neighboring joint and subsequently the dressing slipped. Only 1 patient developed Koebner response at the donor site. None of our patients had milia formation or scarring. In patients with stable vitiligo, autologous melanocyte transfer is a simple and effective technique to produce homogeneous pigmentation quickly. It has an advantage over conventional split thickness grafting as it requires very little donor skin (usually only one tenth of the recipient site).[9] Patients were generally satisfied with the results as the quality of repigmentation was superior. Further large scale patient studies are required, especially with melanocyte culture methods, to confirm the efficacy of autologous melanocyte transfer techniques[12]. References
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05131f1.jpg] [dv05131t4.jpg] [dv05131t2.jpg] [dv05131t3.jpg] [dv05131t1.jpg] [dv05131f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}