 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 6, November-December, 2005, pp. 401-405 Original Article A comparative evaluation of skin and nerve histopathology in single skin lesion leprosy Reddy RaghunathaR, Singh Gurcharan, Sacchidanand S, Okade Rajendra, V Shivakumar, A Uday, Haneef NayeemSadath Department of Dermatology and STD, SriDevaraj Urs Medical College, Tamaka, Kolar, Karnataka Code Number: dv05133 Abstract Background: In spite of leprosy being a disease of nerves, ROM therapy for single skin lesion leprosy was based on clinical trials without much evidence-based studies of nerve pathology. The present study was undertaken to compare the histology of skin and nerve in single skin lesion leprosy, and to assess the scientific rationale and justification of single dose ROM therapy. Keywords: Single skin lesion Hansen′s disease, ROM therapy, Nerve biopsy Introduction In 1997, based on WHO recommendations, India and other countries implemented ROM therapy, rifampicin 600 mg, ofloxacin 400 mg and minocycline 100 mg as a single dose, for patients with single skin lesion leprosy without clinically thickened peripheral nerves.[1] Some clinical trials of single dose ROM therapy for all PB cases have subsequently been conducted with encouraging results, but all are with soft targets like resolution or disappearance of skin lesions.[2] There are few studies based on pathological evidence of the disease and with a follow up period being sufficient to determine the rate of reactions, relapses and recurrences. Leprosy can be therapeutically better served if the following golden rules are considered:
This study was started based on these facts and aimed
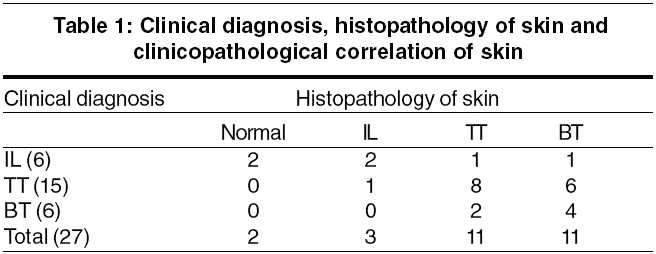
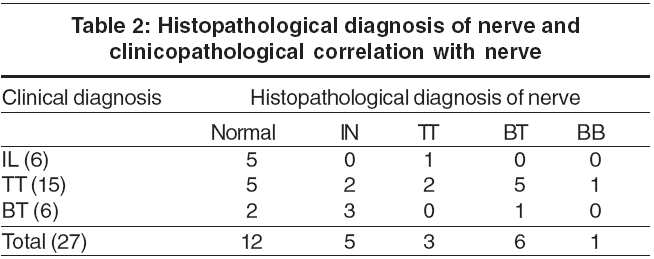
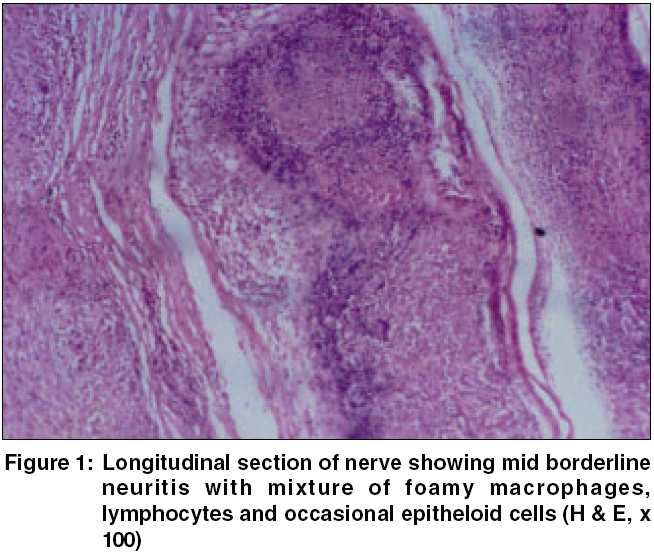
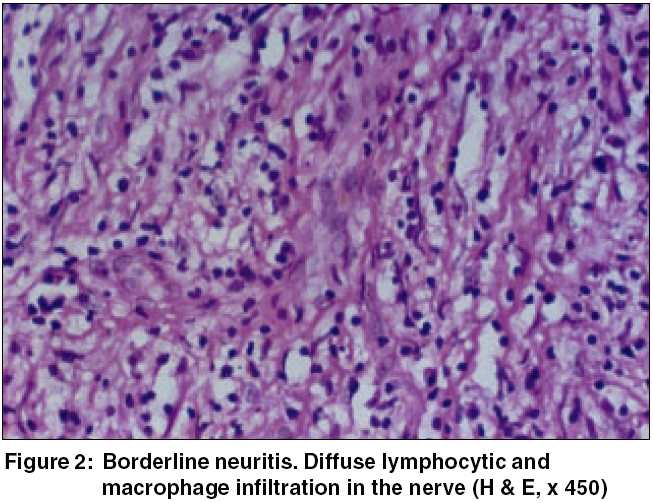
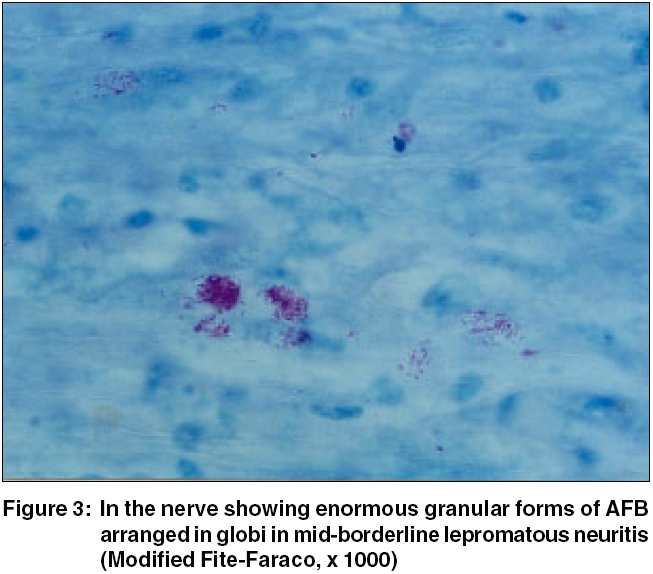
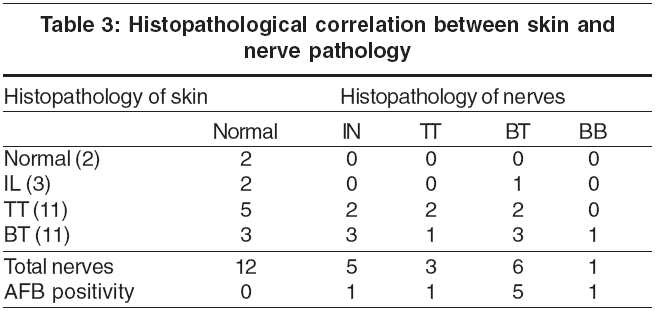
Methods Twenty-seven untreated leprosy patients having a single skin lesion located near the radial cutaneous, sural or great auricular nerves, without significantly thickened peripheral nerves, were selected randomly from the Departments of Dermatology and STD of Victoria Hospital, Bangalore, SNR District Hospital and RL Jalappa Hospital and Research Centre, Kolar, during the period November 1998 to January 2003. Biopsies from skin lesions over the lower half of the forearm, lower leg, neck and inferolateral aspect of the face and from nearby pure cutaneous nerves were studied under both H and E and Fite′s stains. Nerve biopsy procedure After these incisions, blunt dissection was done carefully, upto the level of the subcutis. The nerve was identified and freed for a length of about 3 cm. An artery forceps was introduced beneath the nerve trunk and its blades were separated. Both the ends of the nerve were tied. The nerve trunk was split along the length and a partial or full thickness of 2.5-3 cm length of the nerve was biopsied. The wound was sutured in layers. The specimen was preserved in 10% formaldehyde solution and sent for histopathological examination. Results Twenty-seven patients, 19 males and 8 females, were included in this study. The youngest patient was 7 years old and the oldest was aged 68 years; the maximum number of patients was in the age group of 25-35 years. Four patients had skin lesions over the face and neck, 9 over the lower limbs and 14 over the upper limbs. The duration of the lesions varied from 1 month to 14 months. Sensations over the skin lesions were intact in 11, decreased in 7 and absent in 9 patients. A clinical diagnosis of tuberculoid leprosy (TT) was made in 15 patients, borderline tuberculoid (BT) leprosy in 6 patients, and indeterminate (IL) leprosy in 6 patients. Histopathology of the skin with clinico-pathological correlation [Table - 1] : Clinico-pathological correlation with the skin biopsy findings was seen in 14 out of 27 cases (51.85%). All the skin biopsies were negative for AFB. Histopathology of the nerve with clinico-pathological correlation of nerve [Table - 2]: The histopathological diagnosis of Hansen′s disease was evident in 55.5% (15/27) of nerve biopsy specimens, where the nerves were clinically not significantly thickened [Figure - 1][Figure - 2] [Figure - 3]. Histopathological correlation between skin and nerve [Table - 3]: Histopathological correlation between the skin and nerve findings was seen only in 26% (7/27) of cases. AFB were demonstrated in 29.6% (8/27) of nerve biopsies with formation of globi in 3 cases. An inflammatory infiltrate diagnostic of leprosy was seen in 55.5% cases in nerve biopsies. Discussion The incidence of leprosy, especially infective cases, has reduced drastically after the introduction of MDT, and yet leprosy continues to be a major public health problem. Active case detection programs show an increase in the number of single lesion cases.[3] Leprosy is primarily a disease of nerves even though most of the criteria for diagnosis are related to the skin.[4] Pathologically, more than 30% of the nerve should be involved for functional impairment to be appreciated clinically. The entire spectrum of leprosy has been observed in nerves. Lepromatous morphology is not uncommon even in patients with thickening of a single nerve. Recent histological studies have shown deep dermal nerve involvement even in indeterminate leprosy patients. Distant uninvolved nerves may also show evidence of the disease. [5] While the skin histology continues to be the standard tool in confirming the diagnosis and classification of leprosy, the nerve histology gives more information about the exact classification.[4],[6] Several authors have observed differences in the bacillary load and in the histopathology between the skin and nerve lesions, particularly in PB cases.[7] In early lesions there appears to be a dichotomy in immunological grading between the skin and nerve and this needs to be explored in greater detail. The majority of reports show discordance between skin and nerve histology, showing immunologically lower spectrum of disease in nerves. Mukherjee and Misra, in a study of comparative histopathology of skin and nerve granulomas in leprosy patients showed high granuloma fraction, caseation and increased extent and severity of the disease in nerves.[8] In one report, viable bacilli were detected (by injecting suspensions into the mouse footpad) in 33% of nerve biopsies and in 19% of skin biopsies of patients after 2 years of treatment with MB-MDT.[9] A similar study from Hyderabad concluded that further studies are needed to determine the relevance of skin and nerve histology and the presence or absence of AFB in the nerves to determine the correct duration of therapy.[10] Several other studies have also shown differences in the histopathological findings of skin and nerve biopsies.[11] The nerves were found to be bacillated even after the skin lesions had cleared or regressed.[11] A nerve biopsy is more informative and specific than a skin biopsy in the diagnosis and classification of patients when the skin histology is indeterminate.[4],[6] ROM has been accepted and implemented the world over. It is claimed to be successful in patients with single skin lesion leprosy without thickened peripheral nerves. Since the assessment and cure criteria are slightly controversial, it is difficult to decide the endpoint of treatment in neuritic leprosy. Several patients show advanced disease and are AFB positive in both the skin and the nerve even when only one or a few nerves are clinically affected. This suggests that such patients are better included in the MB group, whereas the WHO recommends PB-MDT for such patients.[12] ROM therapy has been found to be operationally attractive, feasible and acceptable to the community, but several leprologists have reservations with specific reasons against the concept of single dose ROM therapy.[13] A double blind, placebo-controlled multicenter trial in India with ROM and PB-MDT for single skin lesion leprosy found clinical improvement to the same extent in both groups.[14] The ROM group showed 46.9% complete cure compared to 54.7% in the PB-MDT group. In this study, the measures of outcome were soft, like clinical improvement and complete clearance of lesions. Encouraged by these results, the NLEP adopted single dose ROM therapy for PB patients with 2-3 skin lesions. The results were almost similar in the patients who had lesions in the same anatomical region, but PB-MDT gave better results in patients who had lesions in different anatomical sites. This clearly suggests that apart from the number of skin lesions there are several other factors to be considered. In this study, the sample size was small, the duration of observation was only 18 months, and, most importantly, there was no information on the relapse rate.[14] Another study conducted by the same group in a large number of PB patients with 1-5 skin lesions, with treatment for 6 months and follow up for 4 years, is expected to generate more information on cure and relapse rates.[2] Disappearance of the granuloma was seen in 70% in ROM + Convit vaccine group, but in only 53.3% with ROM alone, which is statistically significant.[15] Recently, a WHO technical advisory group reviewed the preliminary findings of ROM trials for single skin lesion PB cases, and PB cases up to 5 skin lesions. They recommended an additional year of follow up together with full analysis of findings for the programme.[16] Leprosy is essentially neural in inception and exhibits lower immunological grading and higher bacterial load in nerves as compared to skin, as evident in the present study. Even though a nerve biopsy is not feasible and practical in the field and in mass control programs, the utility of neural histology in selecting and monitoring therapeutic regimens to prevent drug resistance and relapse can not be overemphasized, since neural histology gives better information about classification as it is evidenced by the findings in this study. References
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05133t2.jpg] [dv05133t3.jpg] [dv05133t1.jpg] [dv05133f3.jpg] [dv05133f2.jpg] [dv05133f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}