 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
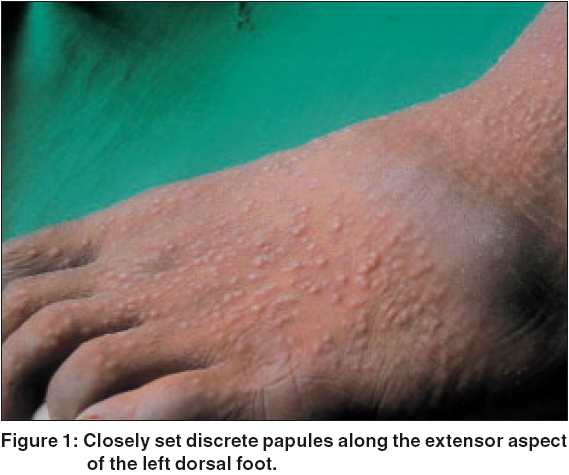
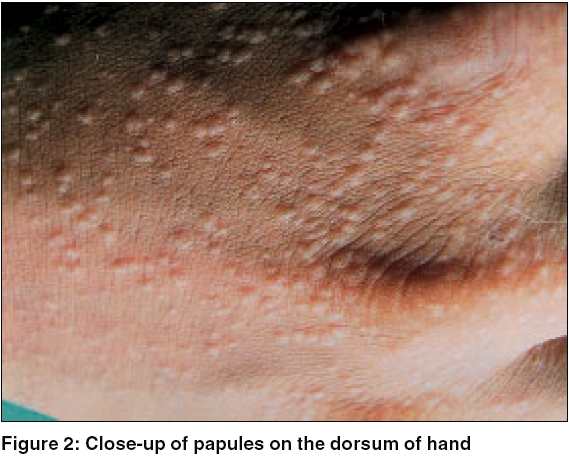
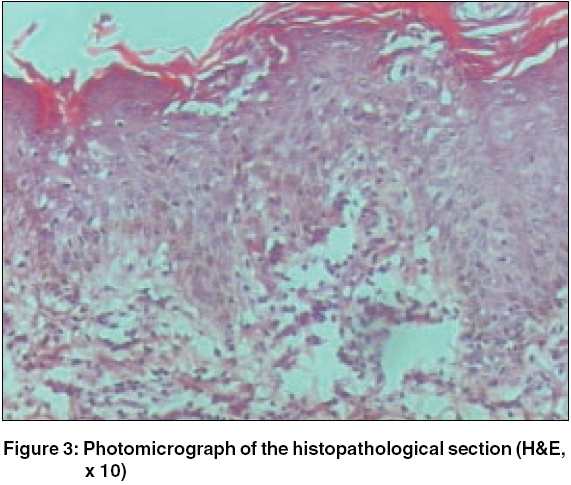
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 6, November-December, 2005, pp. 447-448 Quiz Acral papular eruption Nikam Balkrishna, Amladi Sangeeta, Bingewar Ganesh, Nayak Chitra, Wadhwa SL Department of Dermatology, T N Medical College and B Y L Nair Hospital, Mumbai Code Number: dv05149 A 16-year-old boy presented with a sudden onset of asymptomatic skin eruption since the past seven days. The lesions initially appeared on the thighs and lower legs, followed by ankles, hands, forearms, feet and progressed to elbows, arms and ear lobes. He also complained of decreased appetite, high colored urine and yellowish discoloration of the eyes since the last two weeks. On examination, there were multiple skin colored to erythematous and edematous papules of about 1 to 5 mm size [Figure - 1]. Many of the lesions, located over the extensor aspects of hands [Figure - 2], forearms, elbows and upper arms were topped with tiny crusts and scales whereas others showed a central dusky hue. Examination of the conjunctiva revealed mild icterus. Bilateral axillary, epitrochlear and inguinal nodes were enlarged, non tender, mobile and firm. There was no hepato-splenomegaly. A skin biopsy taken from a papule is presented in [Figure - 3]. On further investigation, he was found to have deranged liver function tests with total bilirubin 1.7 mg%, SGOT 230 U/l, SGPT 375 U/l and serum alkaline phosphatase 502 U/l. He was tested positive for HBsAg. What is your diagnosis? Histopathological findings: Diagnosis: Gianotti Crosti Syndrome (GCS) Treatment and follow-up Discussion GCS, also known as papular acrodermatitis of childhood, (Gianotti and Crosti, 1955) is a widespread infectious disease seen in childhood.[1] It is characterized by a non-relapsing erythemato-papular dermatitis lasting for about 3 weeks, para-cortical hyperplasia of the lymph nodes, acute hepatitis, usually anicteric, lasting for a minimum period of 2 months and hepatitis B surface antigenemia.[1] Following the initial report, subsequent cases have been found to be associated with a wide range of viruses such as hepatitis B and A virus , Epstein Barr virus , Coxsackie A16 , B4 and B5, echovirus, polio virus, cytomegalovirus, respiratory syncytial virus, parainfluenza virus, parvovirus and human immunodeficiency virus .[2],[3] The term GCS has now been accepted to include all acrally located eruptive dermatoses clinically characterized by papular or papulovesicular lesions caused by different viruses and running a benign, self limiting course.[4] The condition appears to be a cutaneous response to viral infection that regresses spontaneously. The clinical manifestations are variable with individual patient characteristics rather than the associated virus.[4] GCS[1] mainly affects children between the ages of 6 months to 12 years, though rarely adults can be the sufferers. The eruption consists of monomorphic, flat, lentil-sized, erythemato-papular, non-itchy lesions symmetrically distributed over face, buttocks and limbs. The lesions may be dense but do not coalesce and occasionally become purpuric, especially over the lower legs. Onset of the rash is acute over a few days and lasts for 2 to 8 weeks with spontaneous regression. Recurrences are unlikely. Lymph nodes, mainly axillary and inguinal, are moderately enlarged, firm and freely movable and may persist for 2 to 3 months. Biopsy of the skin lesion shows hyperkeratosis with mild to moderate acanthosis, papillary dermal edema and superficial perivascular infiltrate of mononuclear cells and histiocytes. Diagnosis is usually based on the typical clinical features;[5] however conditions such as papular urticaria, scabies, lichen planus, hand-foot-mouth disease, erythema multiforme, pityriasis lichenoides and Henoch-Schonlein purpura may have to be differentiated.[5] Extensive truncal and scaly lesions are proposed to be negative clinical features. No treatment is required for the skin lesions. Patients suffering from hepatitis B need prolonged treatment and follow-up. In hepatitis-associated GCS,[1] the patient is usually anicteric. However, icterus may develop concurrent with the rash or after its subsidence. Moderate hepatomegaly and deranged liver function tests may be seen and HBsAg may be positive. Changes in the laboratory parameters usually persist for 1-3 months but in 50% cases, may persist for years. References
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05149f3.jpg] [dv05149f2.jpg] [dv05149f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}