 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
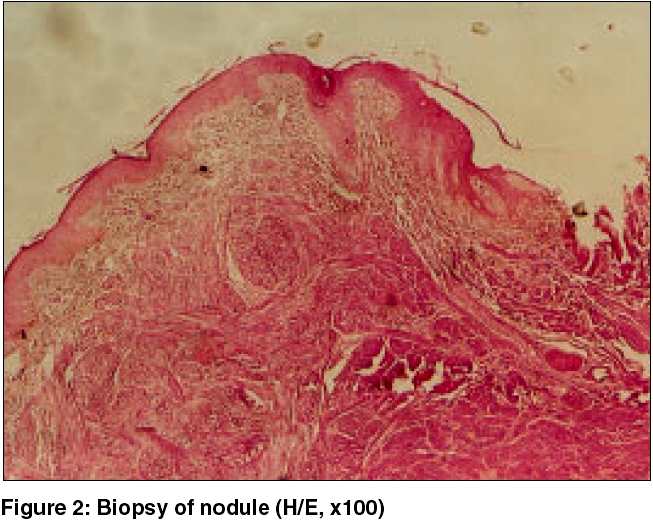
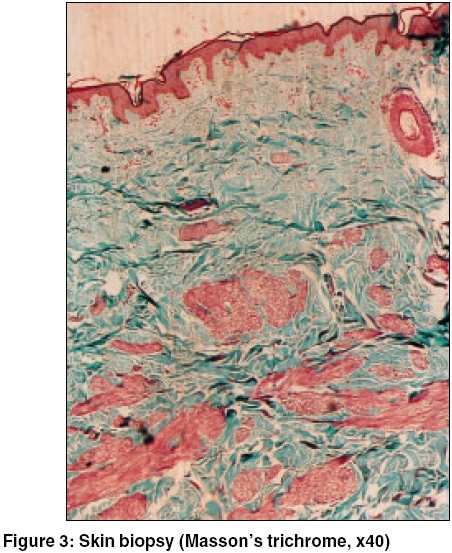
Indian Journal of Dermatology, Venereology and Leprology, Vol. 71, No. 6, November-December, 2005, pp. 449-451 Quiz Multiple painful nodules Rai VandanaMehta, Balachandran C, Kudva Ranjini Department of Skin and STD,Kasturba Hospital, Manipal Code Number: dv05150 A 49-year-old lady presented with multiple painful reddish brown nodules over the body since the age of 15 years. At onset there was only one nodule on the left scapula that gradually increased in size associated with pain on tactile stimulus. Later, over the course of years, she developed multiple small reddish-brown papulonodules on the left forearm, left gluteal region [Figure - 1], and face, and on the right breast around the areola. On further questioning, she gave a history of having undergone hysterectomy a few years back due to nodules in the uterus. There was no history of similar lesions in her mother or sister. All routine investigations such as hemogram, urine analysis, liver and renal function tests, chest X-ray, and ultrasonography of abdomen were normal. A biopsy from one of the new nodules showed spindle shaped smooth muscle cells with cigar shaped nuclei arranged in fascicles and whorls, with a sparse lymphocytic infiltrate in the interstitium, thus confirming the diagnosis of piloleiomyoma [Figure - 2] [Figure - 3]. What is your diagnosis? Diagnosis: Myomatosis cutis et uteri (Reed syndrome)Discussion Women with multiple piloleiomyomas may have uterine leiomyomas. If the latter are present, the patient is likely to have a familial condition called as familial myomatosis cutis et uteri or Reed syndrome, which is inherited as an autosomal dominant trait with incomplete penetrance. [1],[2],[3] In such cases, a uterine myoma requires careful monitoring since it is associated with a significant risk of gynecological complications. Fumarate hydratase, a component of the tricarboxylic acid cycle, acts as a tumor suppressor gene. Germline mutations in the fumarate hydratase gene predispose to multiple cutaneous and uterine leiomyoma syndrome.[4] Mutations are found in 75% cases of multiple cutaneous and uterine leiomyoma syndrome. Leiomyomas are benign soft tissue tumors that may originate from the arrector pili muscle of hair follicles (piloleiomyomas), tunica dartos of the scrotum, mammillary muscle of the nipple (genital leiomyomas), and the smooth muscles of blood vessels (angioleiomyoma).[5] Piloleiomyomas generally occur in the age group of 10-30 years. They may be solitary or multiple and present clinically as erythematous to brown colored papulonodules located over the extensor extremities, trunk, neck and face. The most common feature in patients with multiple piloleiomyomas is pain, which may be induced by cold, tactile and emotional stimuli. Because piloleiomyomas develop in the superficial dermis, they are fixed in the skin; however, they can be moved easily over the deeper subcutaneous tissues. Piloleiomyomas can develop sporadically or be transmitted genetically.[6] They may even occur in a dermatomal or linear pattern.[7] Angioleiomyomas present as a solitary skin colored nodule on the lower extremities. They too are often painful. The pathogenesis of pain associated with these lesions is a mystery. Some authors suggest it is due to local pressure by the tumor on the neurofibrils or due to constriction of the vessels, causing local ischemia.[8] Genital leiomyomas arise from the dartos muscle of the scrotum or from the smooth muscle of the labia majora. They are usually asymptomatic and range in size from a few millimeters to a few centimeters. Leiomyomas are benign tumors and medical management has a limited role. Calcium channel blockers, particularly nifedipine, relieve pain associated with piloleiomyomas.[9] They act by inhibiting the movement of extracellular calcium ions across the cell membrane into the smooth muscle cell, thereby inhibiting muscular contraction. Besides this, phenoxybenzamine[10] and gabapentin[11] have also been tried for piloleiomyomas associated pain. Surgical excision is effective in solitary cases. CO2 laser ablation has been tried in multiple leiomyomas.[12] References
Copyright 2005 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv05150f3.jpg] [dv05150f2.jpg] [dv05150f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}