
|
Indian Journal of Dermatology, Venereology and Leprology
Medknow Publications on behalf of The Indian Association of Dermatologists, Venereologists and Leprologists (IADVL)
ISSN: 0378-6323 EISSN: 0973-3922
Vol. 72, Num. 2, 2006, pp. 119-125
|
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 119-125
Original Article
Cutaneous manifestations in patients with chronic renal failure on hemodialysis
Udayakumar P, Balasubramanian* S, Ramalingam KS†, Lakshmi Chembolli, Srinivas CR, Mathew AnilC‡
Departments of Dermatology, *Nephrology and ‡Community Medicine, PSG Hospitals, Peelamedu, Coimbatore, India; †Coimbatore Kidney Centre, Coimbatore, Tamil Nadu, India.
Correspondence Address:Dr. C. R. Srinivas, Department of Dermatology, PSG Hospitals, Peelamedu, Coimbatore 641 004, Tamil Nadu, India. E-mail: srini_cr_1955@yahoo.com
Code Number: dv06037
Abstract
Background: Chronic renal failure (CRF) presents with an array of cutaneous manifestations. Newer changes are being described since the advent of hemodialysis, which prolongs the life expectancy, giving time for these changes to manifest.
Aim: The aim of this study was to evaluate the prevalence of dermatologic problems among patients with chronic renal failure (CRF) undergoing hemodialysis.
Methods: One hundred patients with CRF on hemodialysis were examined for cutaneous changes.
Results: Eighty-two per cent patients complained of some skin problem. However, on examination, all patients had at least one skin lesion attributable to CRF. The most prevalent finding was xerosis (79%), followed by pallor (60%), pruritus (53%) and cutaneous pigmentation (43%). Other cutaneous manifestations included Kyrle's disease (21%); fungal (30%), bacterial (13%) and viral (12%) infections; uremic frost (3%); purpura (9%); gynecomastia (1%); and dermatitis (2%). The nail changes included half and half nail (21%), koilonychia (18%), onychomycosis (19%), subungual hyperkeratosis (12%), onycholysis (10%), splinter hemorrhages (5%), Mees' lines (7%), Muehrcke's lines (5%) and Beau's lines (2%). Hair changes included sparse body hair (30%), sparse scalp hair (11%) and brittle and lusterless hair (16%). Oral changes included macroglossia with teeth markings (35%), xerostomia (31%), ulcerative stomatitis (29%), angular cheilitis (12%) and uremic breath (8%). Some rare manifestations of CRF like uremic frost, gynecomastia and pseudo-Kaposi's sarcoma were also observed.
Conclusions: CRF is associated with a complex array of cutaneous manifestations caused either by the disease or by treatment. The commonest are xerosis and pruritus and the early recognition of cutaneous signs can relieve suffering and decrease morbidity.
Keywords: Chronic renal failure, Hemodialysis
Earlier diagnosis and treatment of patients with CRF improves the quality of life and prolongs the life expectancy of these patients, giving time for newer cutaneous manifestations to develop. In a study by Pico et al., all the patients with CRF had one or more skin manifestations,[1] while Bencini et al. noticed skin changes in 79% of patients.[2] Our study was conducted to determine the prevalence of cutaneous alterations in CRF patients on hemodialysis.
Methods
One hundred successive patients of CRF undergoing hemodialysis were examined
for cutaneous manifestations in a tertiary hospital. Patients undergoing hemodialysis
following a renal transplant failure or those who had undergone peritoneal
dialysis were not included. The patients′ age, sex, primary and secondary diagnoses, medications and present cutaneous illnesses were noted. A detailed history with regard to duration of CRF, duration of dialysis, duration of skin ailment, onset of changes with relation to diagnosis of CRF and starting dialysis and improvement noticed following dialysis was recorded. Specific investigations like skin biopsy, culture and sensitivity for bacterial infections, Gram′s
stain, potassium hydroxide mount and fungal culture were done where indicated,
after informed consent. Routine investigations for monitoring renal functions
were recorded. The severity of xerosis was assessed by a modified version of
the grading by Morton[3]: grade
0 (smooth skin), grade 1 (rough skin) and grade 2 (rough skin with scaling).
Statistical analysis was done using Chi-square test or Fisher exact test.
The risk (odds ratio) of onychomycosis, half and half nail and acquired perforating
disorder (APD) in diabetes and associated 95% confidence intervals were
estimated using logistic regression analysis with SPSS Software (11.5 version).
Tests with two-sided P values were performed. p value less
than 0.05 was considered as statistically significant.
Results
One hundred patients (70 males and 30 females) were examined. Most of them
were aged between 41 and 50 years; the youngest patient was aged 10 years and
the oldest, 76 years. The duration of chronic renal failure varied from 1 month
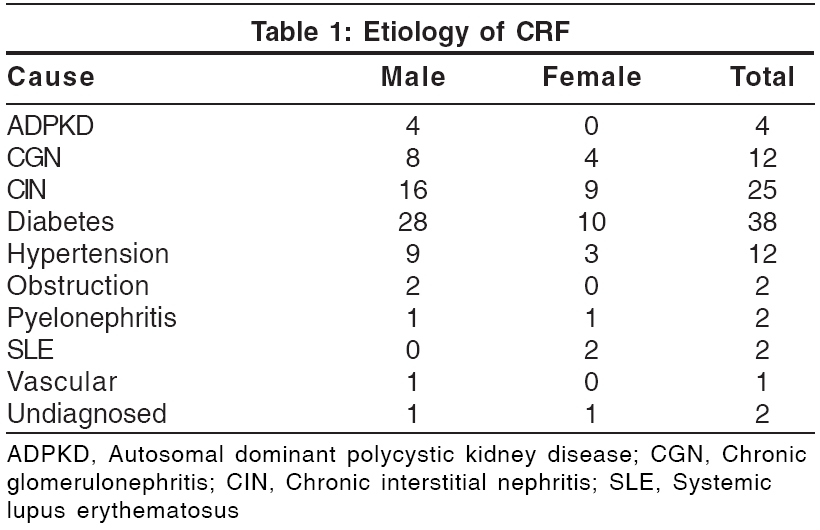
to several years. The various causes leading to renal failure are shown in
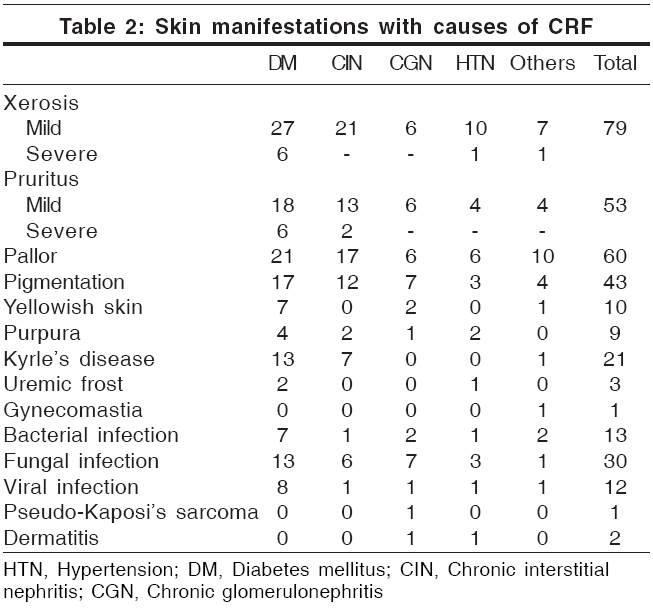
[Table - 1]. Nine patients had a hemoglobin level of less than 5 g%, 58 had 5.1-8 g% and 30 had more than 8 g%. Eleven patients (6 male and 5 female) were HBsAg positive; one patient was HCV positive and one HEV positive. All patients examined in the study showed at least one cutaneous manifestation, although only 82% complained
of some skin problem. Skin manifestations in relation to causes of CRF are
shown in [Table - 2].
Discussion
Xerosis
Xerosis was the most common cutaneous abnormality (79%), as observed in previous reports (46-90%).[4],[5],[6] This
was classified as mild (71%) and severe (8%). Two out of the
79 patients had hypothyroidism and had noticed dry skin prior to the diagnosis
of CRF, while 4 had xerosis from childhood. Thirty-seven patients had associated
keratosis pilaris-like lesions. Xerosis was predominantly seen over the extensor
surfaces of the forearms, legs and thighs. The abdomen and chest showed fine
scaling. Xerosis worsened in 9 patients, improved in 5 patients and was unchanged
in 65 patients while on hemodialysis. It was severe in diabetics . Xerosis is a known complication of diabetes.[6] A reduction in the size of eccrine sweat glands may be contributory, although high dose diuretic regimens are also implicated.[1],[7]
Pruritus
Pruritus is one of the most characteristic and annoying cutaneous symptoms of CRF.[1],[3],[8] It is not present in acute renal failure and does not necessarily subside with dialysis although it improves with kidney transplantation.[8] Its
prevalence among hemodialysis patients ranges from 19 to 90%.[1] In
our study, 53% of patients complained of pruritus. Fifteen (28%) patients had pruritus before the diagnosis of CRF. Thirty-eight out of 53 patients (72%) found no improvement following dialysis, 5 (9.4%) showed improvement and 10 patients (18.8%)
reported aggravation after hemodialysis. It was found to be severe in diabetic
patients.[4] The etiology of pruritus
in CRF is unknown. However, it has been associated to the degree of renal insufficiency
(urine output of < 500 ml);[1],[2] secondary hyperparathyroidism; xerosis[9]; increased serum levels of magnesium, calcium and phosphate, aluminum; increased serum levels of histamine; proliferation of nonspecific enolase-positive sensory nerves in the skin; hypervitaminoses A; and iron deficiency anemia.[4] Slowly accumulated or deposited pruritogen(s), the nature of which is uncertain, are the likely cause.[7] Increased serum histamine levels may be due to allergic sensitization to various dialyzer membrane components and due to impaired renal excretion of histamine. UVB radiation is effective in uremic pruritus.[9] It is thought to act by suppressing histamine-releasing factors in the sera of uremic patients.[10] In addition, UVB also reduces vitamin A levels in the epidermis, suggesting that increased epidermal vitamin A may be contributory.[9] Oral cholestyramine and activated charcoal are other alternatives.[9] The opioid antagonist naltrexone is reported to reduce severe intractable pruritus in hemodialysis patients,[9] but other articles have not found it to be beneficial.[9] Erythropoietin therapy can alleviate pruritus in some cases of CRF.[9] Topical
capsaicin cream (0.025%)[9] and oral ondansetron, a serotonin receptor antagonist, have also been reported to be effective.[9] Recently, low dose gabapentin therapy has been tried in hemodialysis patients with good results.[11]
Pallor
Pallor of the skin due to anemia, reported as the hallmark of chronic
renal failure, was observed in only 60% of patients, possibly because of the darker complexion. The hemoglobin level was less than 8 g% in 64% of
the patients. This is a common early finding and adds significantly to the
mortality.[7]
Pigmentary changes
Two types of pigmentary charges were observed: hyperpigmentation (seen
in 43% of patients) and a yellowish tinge to the skin (10%). Prominent hyperpigmentation over the sun-exposed areas was seen in 26%. Other authors have reported a prevalence of 20-22%.[1],[4] Diffuse hyperpigmentation on sun-exposed areas is attributed to an increase in melanin in the basal layer and superficial dermis due to failure of the kidneys to excrete beta-melanocyte-stimulating hormone (β
-MSH).[12] Hyperpigmented macules on the palms and soles have been reported by Pico et al. and are also attributed to increased circulating β
-MSH.[1],[12] A
yellowish tinge to the skin has been reported in 40% of patients by
other studies[1] but was seen in
only 10% of our patients, probably because their darker complexion masked
the finding. It has been attributed to the accumulation of carotenoids and
nitrogenous pigments (urochromes) in the dermis[13] or the presence of lipochromes and carotenoids in the epidermis and subcutaneous tissue.[14]
Acquired perforating disorders
Perforating disorders such as perforating folliculitis, Kyrle′s
disease and reactive perforating collagenosis have been described in CRF.[15] The
term ′perforating disorder of renal disease′ or ′acquired perforating disorders (APD)′has
been used to describe the hyperkeratotic follicular papules present in these
patients.[15] APD has been reported
to occur in 4.5-17% of patients on hemodialysis.[1],[5],[15] We
encountered Kyrle′s disease in 21 patients (21%); 19 of them
had undergone dialysis for less than 6 months. These changes were significantly
more prevalent in diabetic patients ( P =0.002, [Table - 3]). The association
of diabetes mellitus and perforating disorders has been confirmed by earlier
studies.[4] Trauma to the skin in patients with pruritus secondary to CRF could be the inciting agent in producing these lesions.[13] The unifying feature of the perforating disorders is the trans-epidermal elimination of altered dermal substances.[16] Keratotic pits of the palms and soles have also been reported in hemodialysis patients.[17]
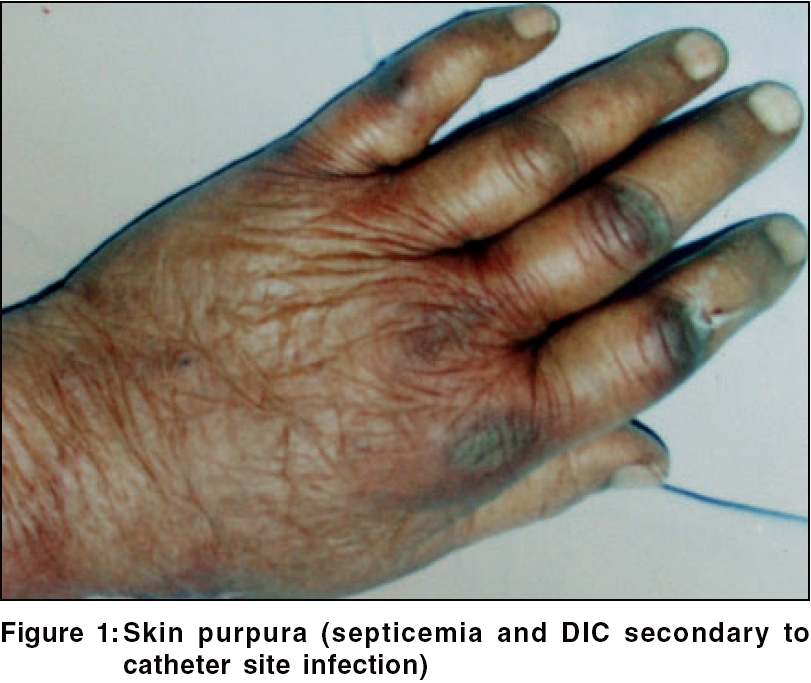
Purpura
Purpura was seen in nine (9%) patients [Figure - 1]. Easy bruising
was reported in a previous study. Singh observed these changes in 20% of
CRF patients not on dialysis.[18] Defects in primary hemostasis like increased vascular fragility, abnormal platelet function and the use of heparin during dialysis are the main causes of abnormal bleeding in these patients.[19]
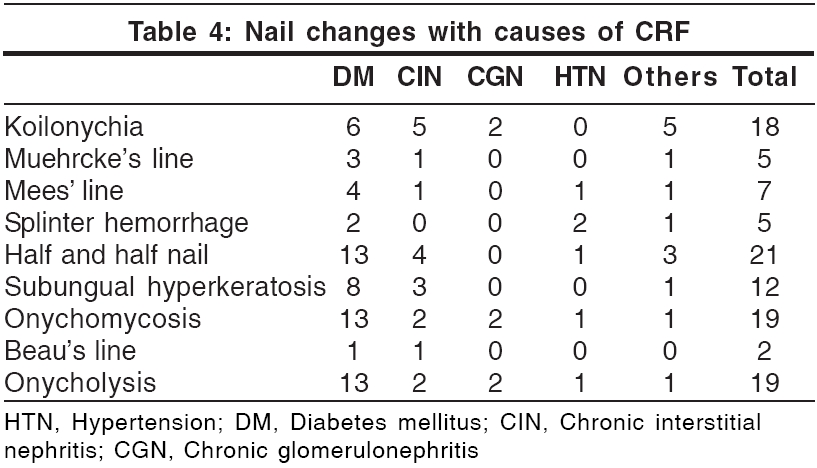
Nail changes [Table - 4]
Lindsay′s nails (half and half nails) are red, pink or brown in
their distal half (this color does not fade with pressure) and white in the
proximal half.[17] This change
was seen in 21% of our patients and was significantly more prevalent
in diabetic patients (p = 0.029; [Table - 4]). Previous studies have found
a prevalence of 16-50.6%.[1],[5] The
prevalence in the general population has been reported to be 1.4%.[1] Other
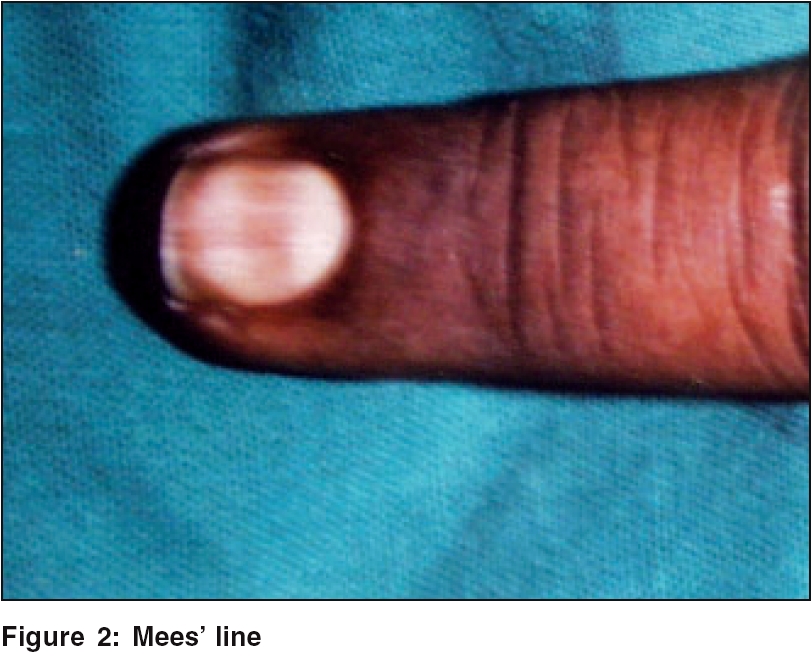
nail changes included koilonychia (18%), subungual hyperkeratosis (12%), onycholysis (10%), Mees′ lines (7%)
[Figure - 2], Muehrcke′s lines (5%), splinter hemorrhages (5%) and Beau′s lines (2%).
Brown nail bed arcs were not seen.
Hair abnormalities
Sparse body hair and diffuse alopecia with dry, lusterless hair have been
reported.[4] In our study, 30 patients
had sparse body hair, 11 had diffuse alopecia and 16 had dry, lusterless hair.
Dry, lusterless hair is due to decreased secretion of sebum.[20] Singh et al. have
reported a prevalence of 30% in CRF patients not on dialysis.[18] Acute
diffuse alopecia following a few weeks of dialysis was reported in 3 patients.[21]
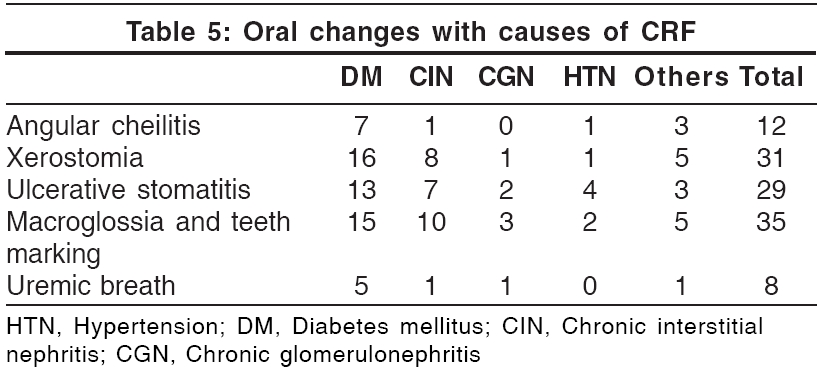
Oral mucosal changes [Table - 5]
Oral mucosal changes have been reported in up to 90% patients with CRF.[22] Teeth
marking with macroglossia (′tongue sign of uremia′) was seen in 35% patients. This finding was first described by Mathew in 92% of
patients with CRF.[23] Xerostomia
was seen in 31 patients (31%). It was attributed to mouth breathing
and dehydration. Ulcerative stomatitis, seen in 29 patients, is reported to
occur in patients with blood urea levels greater than 150 mg/100 ml.[22] Out
of the 29 patients, 16 (55.2%) had a predialysis blood urea nitrogen
level of more than 150 mg. However, 20 patients with a blood urea level of
more than 150 mg/100 ml did not show these changes. This could be attributed
to the poor oral hygiene of these patients.[22] Angular
cheilitis was seen in 12 patients and coated tongue in 11 patients. Eight patients
had uremic fetor, including 3 who had a predialysis blood urea level of more
than 200 mg%. Uremic fetor is an ammoniacal odor caused by a high concentration
of urea in the saliva and its breakdown to ammonia. All 3 patients died within
30 days due to inability to continue treatment. Fewer fungiform taste buds,
in addition to the increased urea, contribute to the impairment of taste in
CRF patients.[22],[24]
Cutaneous infection
Sixty-seven skin infections (13 bacterial, 42 fungal and 12 viral), distributed
amongst 40 patients, were seen in this study. Bacterial infections, seen in
13 patients, were common in diabetics. The fungal infections were distributed
among 30 patients (30%). The commonest one was onychomycosis (19%),
which was significantly more prevalent ( p = 0.039; [Table - 3]) in
the diabetic group. Bencini et al. have reported the incidence of fungal
infection in patients undergoing hemodialysis to be 67%.[2] Tinea
pedis, also reported to be common,[1] was
not seen in our study. CRF patients have impaired cellular immunity due to
a decreased T-lymphocyte cell count; this could explain the increased prevalence
of fungal infections.[1] Pityriasis
versicolor was seen in 15 patients (15%). The viral infections included warts (8%), herpes simplex (3%) and herpes zoster (1%).
Uremic frost
Uremic frost, one of the rarer skin changes that can occur in the acute
setting of severe uremia, was seen in three patients. All of them had a pre-dialysis
blood urea level of more than 200 mg / 100 ml. In the pre-dialysis era, uremic
frost was a frequent dermatologic finding, but it is rarely encountered nowadays
due to the wide availability of hemodialysis.[25] The
frost consists of a white or yellowish coating of urea crystals on the beard
area and other parts of the face, neck and on the trunk. It is due to eccrine
deposition of urea crystals on the skin surface of patients with severe uremia .[25] In
erythema papulatum uremicum, large papules and nodules on an erythematous
base are commonly seen over the palms, soles, forearms and face. In two weeks
they desquamate and develop fissures.[25] With
the advent of dialysis, this change is rarely seen.
Iatrogenic manifestations
Arteriovenous shunt dermatitis may be seen in 8% of patients on
long-term hemodialysis.[26] One
of our patients had eczema at the site of an arteriovenous fistula and another
at the site of the insertion of a catheter. Pseudo-Kaposi′s sarcoma was clinically diagnosed in one patient. A few reports have described the occurrence of pseudo-Kaposi′s
sarcoma near an artificially constructed arteriovenous fistula.[27] It
is seen as purplish nodules or papules which slowly evolve into scaly, crusted,
violaceous patches near the arteriovenous fistula. One patient developed cannula
site infection and died of staphylococcal septicemia. Cannulation septicemia
has been reported in 8%.[8] We
saw gynecomastia in one patient, which is lower than the reported incidence
(40%).[28]
Gynecomastia is not observed in uncomplicated chronic renal failure without
regular treatment. It occurs during the early stages of regular dialysis treatment
and is explained on the basis of ′refeeding′after the start of
treatment.[28] As a consequence
of CRF and protein energy malnutrition, pituitary gonadotrophic and testicular
functions remain suppressed and following treatment and increase in daily protein
intake, a ′second puberty′ensues. This may lead to transient
gynecomastia. Our patient with gynecomastia was an adolescent and developed
gynecomastia during the initial weeks of dialysis. The possibility of gynecomastia
secondary to normal puberty cannot be ruled out. One patient developed a carbamazepine-induced
maculopapular rash, which cleared spontaneously following withdrawal of the
drug. There is an increased incidence of drug reactions in uremia because of
administration of simultaneous admisnidtration of multiple drugs and also due
to prolonged half-life of each medication.[25]
Metastatic calcification of the skin in CRF results from secondary or tertiary
hyperparathyroidism.[17] Abnormally
elevated levels of PTH trigger deposition of crystalline calcium pyrophosphate
in the dermis, subcutaneous fat or arterial wall.[13] Calcified
vessels may thrombose acutely, resulting in calciphylaxis, producing symmetrical
livedo reticularis. Nodular calcium deposits, identical to calcinosis cutis,
may occur in the skin or fat.[13]
Skin changes due to immunosuppression include an increased susceptibility
to infections and development of cancerous and precancerous lesions. A prevalence
of 4.5% has been reported by Bencini et al.[2],[4] Basal
cell carcinoma is the commonest form of skin cancer. Multiple actinic keratoses
occur over sun-exposed areas and may progress to squamous cell carcinoma.
Nephrogenic fibrosing dermopathy (NFD), a recently described disorder of
unknown etiology, resembles scleromyxedema in some aspects.[13] Most
affected patients have been on hemodialysis and many have restarted dialysis
after failure of a renal transplant. NFD has also been described in a few patients
with CRF. It is clinically characterized by the progressive development of
erythematous, sclerotic dermal plaques, usually pruritic on the arms and legs,
with sparing of the head and neck. The histopathology of NFD resembles scleromyxedema,
with proliferation of fibroblasts in the dermis and subcutaneous septae accompanied
by increased dermal and septal collagen and mucin.[13] There
is no effective treatment.
Miscellaneous conditions
Other skin lesions observed included dermatosis papulosa nigra (25), acrochordon
(11), prurigo nodularis (8), idiopathic guttate hypomelanosis (7), insulin
induced lipoatrophy (4), vitiligo (3), diabetic dermopathy, melasma (3), fissures
of the feet (3), hyperkeratosis of the sole (2), papular urticaria (2), chronic
dermatitis of leg (2), seborrheic dermatitis of the scalp (2), varicose eczema
(1) and Schamberg′s disease (1). The association of these changes with
renal failure cannot be established.
Conclusion All our 100 CRF patients on hemodialysis showed at least one cutaneous alteration. Patients with end stage renal failure (ESRD) may present with an array of skin abnormalities. With the advent of hemodialysis, the life expectancy of these patients has increased, giving time for more and newer cutaneous changes to manifest. Some prophylactic and remedial measures can prevent or decrease some of the adverse changes. These include emollients for xerosis; sunscreens, sun avoidance measures and clothing for pigmentary changes and cutaneous malignancies; oral hygiene to prevent oral mucosal changes; nutritional supplementation to prevent vascular fragility, angular cheilitis and hair loss; and prompt recognition and treatment of fungal infections like onychomycosis and tinea pedis, which are increased in CRF.
References
| 1. | Pico MR, Lugo-Somolinos A. Cutaneous alterations in patients with chronic renal failure. Int J Dermatol 1992;31:860-3. Back to cited text no. 1 |
| 2. | Bencini PL, Montagnino G, Citterio A, Graziani G, Crosti C, Ponticelli C. Cutaneous abnormalities in uremic patients. Nephron 1985;40:316-21. Back to cited text no. 2 [PUBMED] |
| 3. | Ponticelli C, Bencini PL. The skin in uremia. In: Massry SG, Glassock RJ, editors. Massry's and Glassock's Textbook of Nephrology. 2nd ed. Williams and Wilkins: Baltimore; 1989. p. 1422-6. Back to cited text no. 3 |
| 4. | Morton CA, Lafferty M, Hau C, Henderson I, Jones M, Lowe JG. Pruritus and skin hydration during dialysis. Nephron Dial Transplant 1996;11:2031-6. Back to cited text no. 4 [PUBMED] |
| 5. | Tawade N, Gokhale BB. Dermatologic manifestation of chronic renal failure. Indian J Dermatol Venereol Leprol 1996;62:155-6. Back to cited text no. 5 |
| 6. | Siddappa K, Nair BK, Ravindra K, Siddesh ER. Skin in systemic disease. In: Valia RG, Valia AR, editors. IADVL Textbook and atlas of dermatology. 2nd ed. Bhalani Publishing House: Mumbai; 2000. p. 938-84. Back to cited text no. 6 |
| 7. | Weisman K. Graham RM. Systemic disease and the skin. In: Champion RH, Burton JL, Burns DA. Breathnach SM, editors. Rook/ Wilkinson/ Ebling Textbook of dermatology. 6th ed. Blackwell Science: Oxford; 1998. p. 2703-58. Back to cited text no. 7 |
| 8. | Guptha AK, Guptha MA, Cardella CJ, Haberman HF. Cutaneous associations of chronic renal failure and dialysis. Int J Dermatol 1986;25:498-504. Back to cited text no. 8 |
| 9. | Etter L, Myers SA. Pruritus in systemic disease: Mechanisms and management. Dermatol Clin 2002;20:459-72. Back to cited text no. 9 [PUBMED] |
| 10. | Imazu LE, Tachibana T, Danno K, Tanaka M, Imamura S. Histamine-releasing factors in sera of uremic pruritus patients is a possible mechanism of UV-b therapy. Arch Dermatol Res 1993;285:423-7. Back to cited text no. 10 [PUBMED] |
| 11. | Manenti L, Vaglio A, Costantino E, Danisi D, Oliva B, Pini S, et al. Gabapentin in the treatment of uremic atch: An index case and a pilot evaluation. J Nephrol 2005;18:86-91. Back to cited text no. 11 |
| 12. | Smith AG, Shuster S, Thody AJ, Alvarez-Ude F, Kerr DN. Role of the kidney in regulating plasma immunoreactive beta-melanocyte stimulating hormone. Br Med J 1976;1:874-6. Back to cited text no. 12 [PUBMED] |
| 13. | Sweeney S, Cropley TG. Cutaneous changes in renal disorders. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Fitzpatrick's Dermatology in general medicine. 6th ed. Mc Graw-Hill: New York; 2003. p. 1622-4. Back to cited text no. 13 |
| 14. | Comaish JS. Ashcroft T, Kerr DN. The pigmentation of chronic renal failure. J Am Acad Dermatol 1975;55:215-7. Back to cited text no. 14 |
| 15. | Heilman ER, Friedman RJ. Degenerative diseases and perforating disorders. In: Elder D, Elenitsas R, Jaworsky C, Johnson Jr. B, editors. Lever's histopathology of the skin. 8th ed. Lippincott-Raven: Philadelphia; 1997. p. 341-51. Back to cited text no. 15 |
| 16. | Lebwohl M. Acquired perforating disorders. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA. Katz SI, editors. Fitzpatrick's Dermatology in general medicine. 6th ed. Mc Graw-Hill: New York; 2003. p. 1041-5. Back to cited text no. 16 |
| 17. | Rustad OJ, Corwing VJ. Punctate keratosis of the palms and soles and keratotic pits of the palmar creases. J Am Acad Dermatol 1990;22:468-76. Back to cited text no. 17 |
| 18. | Singh G, Singh SJ, Chakrabarthy N, Siddharaju KS, Prakash JC. Cutaneous manifestations of chronic renal failure. Indian J Dermatol Venereol Leprol 1989;55:167-9. Back to cited text no. 18 |
| 19. | Remuzzi G. Bleeding in renal failure. Lancet 1988;28:1205-8. Back to cited text no. 19 |
| 20. | Brenner BM, Lazarus JM. Chronic renal failure. In: Isselbacher KJ, Braunwald E, Wilson JD, Martin JB, Fauci AS, Kasper DL, editors. Harrison's Principles of internal medicine. 13th ed. New York: McGraw-Hill; 1994. p. 1274-81. Back to cited text no. 20 |
| 21. | Kint A, Bussels L, Fernandes M, Ringoir S. Skin and nail disorders in relation to chronic renal failure. Acta Derm Venereol 1974;54:137-40. Back to cited text no. 21 [PUBMED] |
| 22. | Cohen GS. Renal disease. In: Lynch MA, editor. Burket's Oral medicine: Diagnosis and treatment. 9th ed. Philadelphia: Lippincott-Raven; 1997. p. 487-509. Back to cited text no. 22 |
| 23. | Mathew MT, Rajarathnam K, Rajalaxmi PC, Jose L. The tongue sign of CRF: Further clinical and histopathological features of this new clinical sign of chronic renal failure. J Assoc Phy Ind 1986;34:52. Back to cited text no. 23 |
| 24. | Astback J, Fernstrom A, Hylander B, Arvidson K, Johansson O. Taste buds and neuronal markers in patients with chronic renal failure. Perit Dial Int 1999;19:S315-S23. Back to cited text no. 24 [PUBMED] |
| 25. | Scoggins RB, Harlan WR Jr. Cutaneous manifestations of hyperlipidemia and uraemia. Postgrad Med 1967;4:537-45. Back to cited text no. 25 |
| 26. | Goh GL, Phay KL. Arterio- venous shunt dermatitis in chronic renal failure patients on haemodialysis. Clin Exp Dermatol 1988;13:1038-40. Back to cited text no. 26 |
| 27. | Goldblum OM, Kraus E, Bronner AK. Pseudo-Kaposi's sarcoma of the hand associated with an acquired, iatrogenic arterio-venous fistula. Arch Dermatol 1985;121:1038-40. Back to cited text no. 27 [PUBMED] |
| 28. | Lindsay RM, Briggs JD, Luke RG, Boyle IT, Kennedy AC. Gynecomastia in chronic renal failure. Br Med J 1967;4:779-80. Back to cited text no. 28 |
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology
The following images related to this document are available:
Photo images
[dv06037t5.jpg]
[dv06037t3.jpg]
[dv06037t2.jpg]
[dv06037f1.jpg]
[dv06037t4.jpg]
[dv06037f2.jpg]
[dv06037t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}