 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 129-132 Original Article Pattern of skin diseases among migrant construction workers in Mangalore Kuruvila Maria, Dubey S, Gahalaut Pratik Department of Dermatology, Venereology and Leprology, Kasturba Medical College and Hospital, Attavar, Mangalore Code Number: dv06039 Abstract Background: With increasing industrialization, the construction industry provides employment to a large number of skilled and nonskilled workers, many of them migrant workers. Keywords: Contact dermatitis, Dermatoses, Migrant workers Introduction An occupational dermatosis is defined as ′a skin disease that would not have occurred if the patient had not been doing the work of that occupation.′Evidences in favor of an occupational origin are:[1]
Of all the occupational dermatoses, contact dermatitis is the most common, comprising 20-90% of all the cases.[2] In the construction industry, various categories of workers are involved such as masons, helpers, fitters, supervisors, carpenters and painters. The common irritants and sensitizers in the construction industry are:[3]
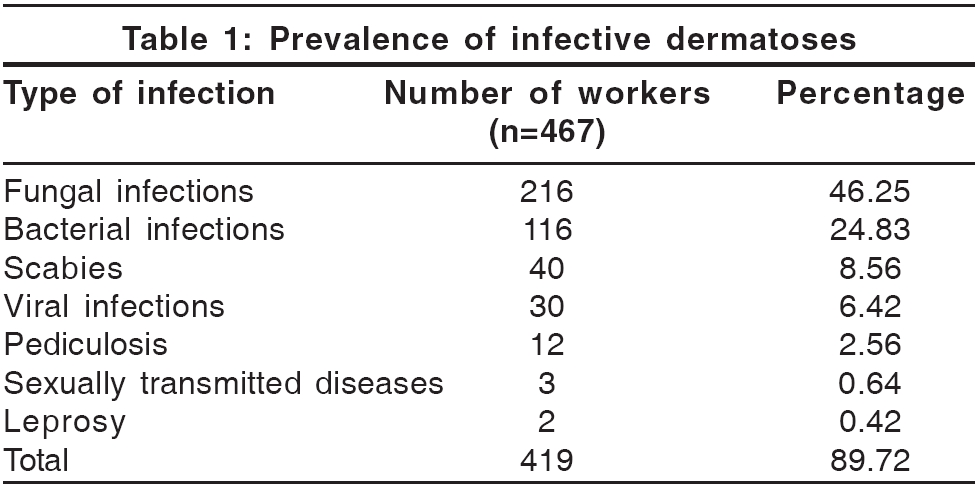
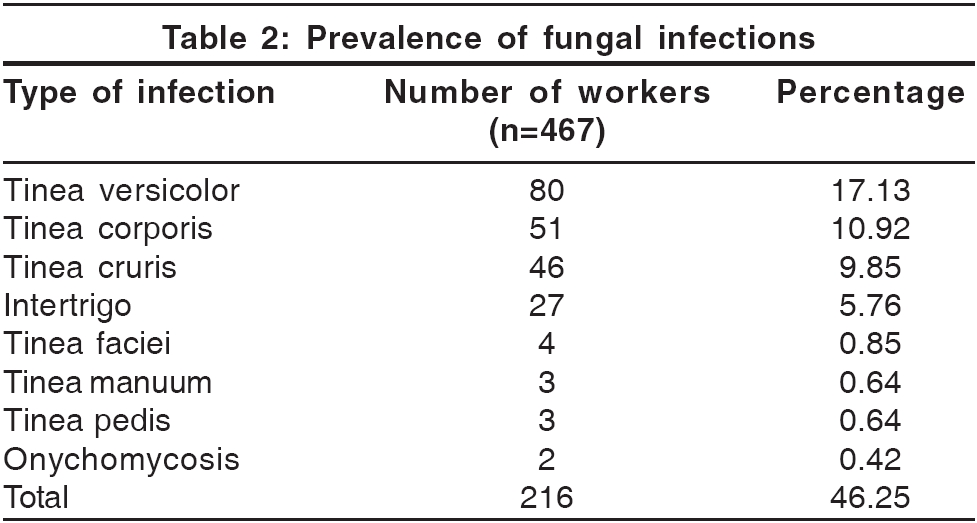
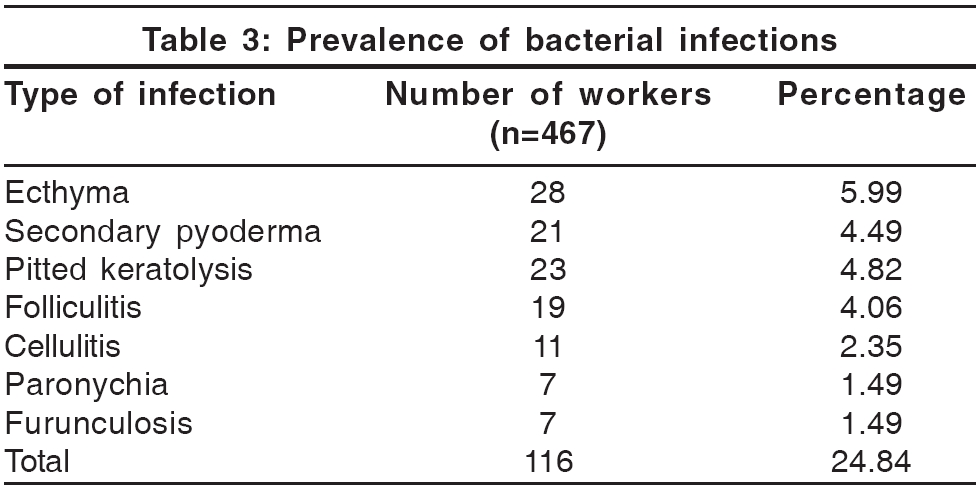
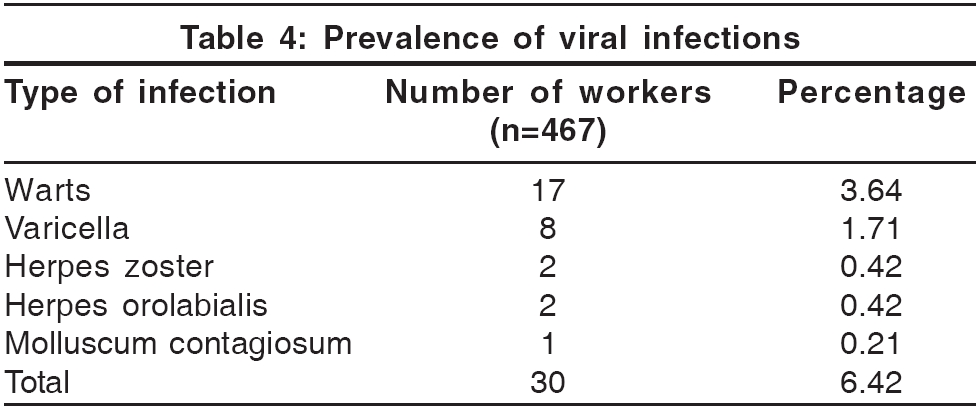
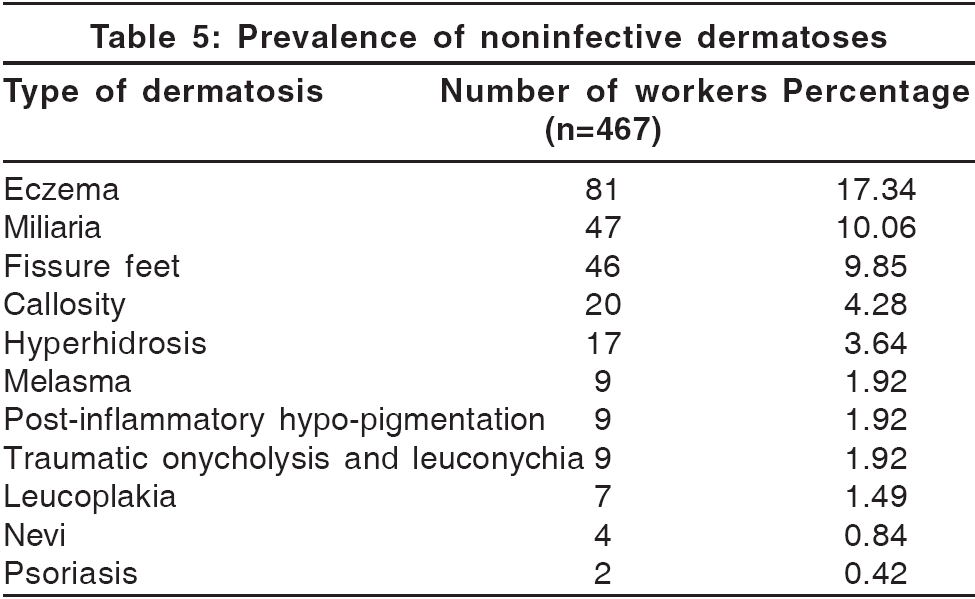
In an earlier study, the prevalence rate of occupational cement dermatitis among cement workers was 37 per 1000.[4] In India, cement has been reported as the most common cause of contact dermatitis.[5] In cement, water-soluble hexavalent chromate is the main allergen, the cobalt in cement acting as a sensitizer. Methods One thousand construction workers at five different construction sites in and around Mangalore were screened for dermatological complaints. After excluding the local laborers, 467 migrant laborers with various dermatoses were assessed. Details of the type of work and materials with which they came in contact were recorded. Based on this, the study group included the following categories: masons, helpers, painters, rod fitters, carpenters, electricians and supervisors. Masons were involved in skilled jobs like laying the bricks and paving and used cement as a basic ingredient in their work. Helpers were involved in unskilled jobs of mixing the cement, carrying it to construction sites, cleaning and helping masons. Each worker was given a complete physical examination in a well-lit examination room at the construction site. The individual cases were diagnosed based on the clinical morphology of the lesions. Patients who required biopsy for confirmation of the diagnosis were referred to specialist referral hospitals. The diagnosis of fungal infection was supported by microscopical examination of potassium hydroxide skin scrapings in suspected cases. Special tests like patch tests and fungal cultures were not done due to financial constraints. Since the study was done in remote construction sites, not all the patients could come to the hospital for review. If the clinical diagnosis was in doubt, only a few workers were referred for a skin biopsy. Moreover, many laborers changed their site of work frequently. Hence, many of them could not be followed up for treatment. Results Four hundred sixty-seven migrant construction workers, including 411 (88%) males, were examined. Of them, 208 (44.53%) laborers belonged to the third decade. The ages of the youngest and oldest laborers were 14 years and 63 years respectively. Only 48 (10.27%) workers were literate. Helpers constituted the major group (51.20%), followed by masons (32.78%). Infective dermatoses were seen in 419 workers (89.72%) and noninfective ones in 251 (53.74%). Prevalence of the various infective dermatoses is detailed in [Table - 1]. A split-up of the figures of the different fungal infections is given in [Table - 2]. Pyogenic bacterial infections of the skin were common [Table - 3] and included ecthyma (5.99%), secondary pyoderma (4.49%), pitted keratolysis (4.82%), folliculitis (4.06%), cellulitis (2.35%), paronychia (1.49%) and furunculosis (1.49%). Out of the two cases of leprosy diagnosed, one each belonged to the borderline lepromatous and borderline tuberculoid spectrum respectively. Chancroid was detected in two patients and lymphogranuloma venereum in one. Among viral infections [Table - 4], warts were the most common (3.64%), followed by varicella zoster infection (1.71%) and others. Four of the eight workers who had chickenpox were from the same construction site. Among noninfective dermatoses [Table - 5], eczema was seen in the maximum number of workers (17.34%), followed by miliaria (10.06%), fissures of the feet (9.85%), callosity (4.28%), hyperhidrosis (3.64%), melasma (1.92%), post-inflammatory hypo-pigmentation (1.92%), leuconychia (1.92%), leukoplakia (1.49%), nevi (0.84%) and psoriasis (0.42%). The most common complaint in those with eczema was itching and burning of the hands and feet during work. Contact dermatitis to cement was the single largest noninfective dermatosis, being seen in 60 (12.48%) workers, followed by polymorphous light eruptions (12 workers, 2.57%), lichen simplex chronicus in (3, 0.64%), atopic dermatitis (2, 0.42%), actinic cheilitis (2, 0.42%) and seborrheic dermatitis (2, 0.42%), Comparison of the two largest groups, i.e., masons and helpers, showed a significantly higher prevalence of contact dermatitis to cement and scabies and viral infections among masons. No statistically significant difference was noted for other dermatoses. Discussion The majority of our workers belonged to the third decade and males outnumbered females. The literacy rate was only 10.27%, which may be a contributory factor for poverty, ignorance and bad environmental hygiene. Infections constituted the commonest dermatoses, particularly fungal infections, probably due to the hot and humid climate in coastal Mangalore. Trauma, increased hydration of skin and maceration provide a suitable environment for the development of dermatophytosis.[6] The high incidence of bacterial infections may be due to unhygienic working conditions at the construction site, the trauma sustained during work and environmental factors such as a hot and humid climate.[7] Scabies may be prevalent because of overcrowding and close contact,[8] as most migrant workers stayed at the construction site. Frequent trauma and close contact may have contributed to the occurrence of warts. An outbreak of chickenpox was detected amongst a family of masons at one construction site, with four cases occurring at the same site. Among noninfective dermatoses, contact dermatitis to cement constituted the highest number of cases. The reported incidence of contact dermatitis to cement ranges from 3.7 to 24%.[5],[9] Contact dermatitis was more prevalent among masons than among helpers, probably because masons come in frequent and more prolonged contact with cement and its products. The high incidence of miliaria and hyperhidrosis may be attributable to environmental factors such as a hot and humid climate. Fissures of the feet may occur because of the dryness of skin, especially in workers who do not wear any protective footwear. Actinic dermatoses like polymorphous light eruption and actinic cheilitis may be attributed to exposure to sunlight without photoprotection. Callosity is a common disorder of keratinization found in manual workers.[10] Conclusion The pattern of dermatoses presented here is an expressive of poverty, ignorance, overcrowding, poor hygiene and exposure to common irritants and sensitizers in the construction industry. Hence, education of workers regarding occupational hazards, improvement in environmental hygiene and provision of cost-effective protective measures (such as clean clothes, adequate bathing facility, footwear and barrier creams) would help reduce morbidity among construction workers.References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06039t5.jpg] [dv06039t3.jpg] [dv06039t2.jpg] [dv06039t1.jpg] [dv06039t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}