 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
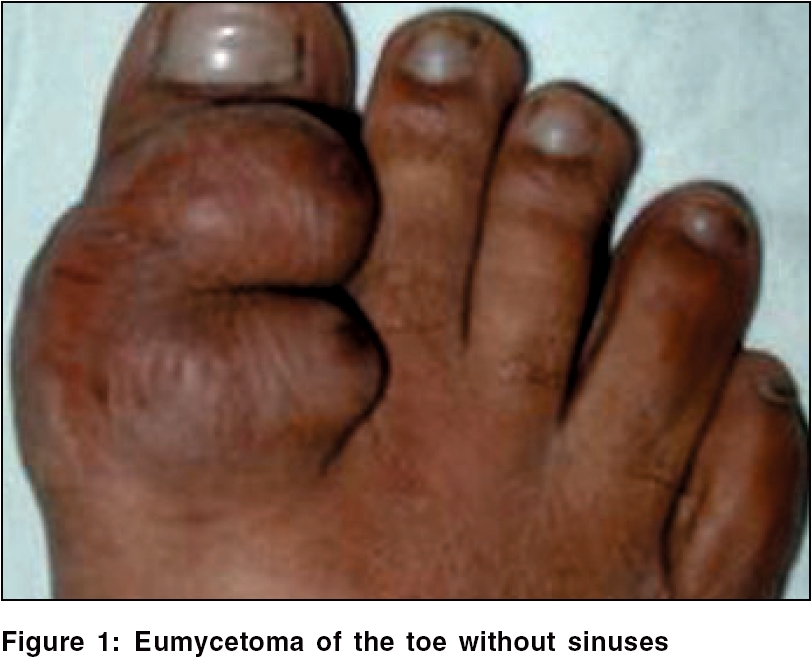
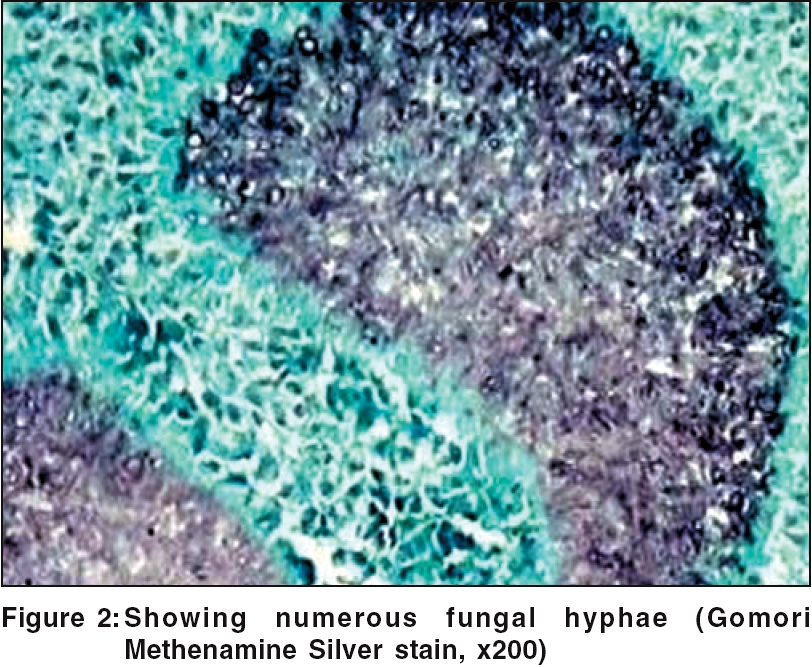
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 143-144 Case Report Mycetoma sans sinuses Saha Sudipta, Dhar Anita, Karak AK* Departments of Surgical Disciplines and *Pathology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India. Code Number: dv06043 Abstract Mycetoma is a chronic suppurative infection involving the skin, subcutaneous tissue and bone. The hallmark of mycetoma is tumefaction, draining sinuses and the presence of microcolonies called grains. Sinuses develop in all patients with mycetoma within a year of the appearance of the lesion. The following case is reported as no sinuses had developed despite the presence of the lesion for 9 years, posing a diagnostic dilemma.Keywords: Chlaymodspores, Mycetoma, Suppurative granuloma Introduction Mycetoma is a disease with a characteristic sign of discharging sinuses.[1] Sinuses develop in all patients with mycetoma within a year of the appearance of the lesion.[2] We report a case of mycetoma without such sinuses. The diagnosis was established after surgical removal of the lesion.Case Report A 50-year-old man presented with a lesion on the right great toe since 9 years. There were no associated symptoms and the lesion was not increasing in size. There was no history of preceding trauma. On examination, there was a 2 x 2 cm (length x breadth) firm, nontender soft tissue swelling over the base of the right great toe with irregular edges [Figure - 1]. There were no clinical signs of inflammation, ulceration, discharge or sinuses. The swelling was free from the underlying bone and tendons. An X-ray revealed no bony involvement. Wedge biopsy from the lesion showed chronic perivascular inflammatory cell infiltration in the dermis. The lesion was excised with primary closure of the defect. Histopathology of the specimen revealed features of mycetoma caused by a true fungus; both fungal hyphae and chlamydospores were present. On H and E staining, numerous sulfur granules were found lying amidst a neutrophilic abscess. Further, numerous fungal hyphae were detected on methenamine staining [Figure - 2]. Discussion Mycetoma is a chronic infectious disease usually involving an extremity. The causal agents generally enter the skin as a result of trauma. The incubation period varies from weeks to several years. Following implantation of the organism, a painless nodule slowly develops and gradually increases in size. The infection typically waxes and wanes from weeks to several years, with the development of recurrent ulceration and multiple draining sinuses and the presence of granules in the discharge. Sinuses seldom develop before 3 months; but about one-third of patients have discharging sinuses by 3 to 6 months and nearly all patients have sinuses by the end of one year.[2] Eventually the infection spreads along the facial planes, extending to deeper structures, leading to bone and joint destruction. The causal agents producing the clinical syndrome can be divided into two classes: actinomycetes and true fungi (eumycetoma). Identification of the cause of mycetoma is based on microscopic examination of granules and isolation of the organisms by culture.[1] Special stains such as PAS and Gomori′s methenamine silver will show hyphae and other fungal structures within the grains.[1] The treatment of mycetoma is difficult. Generally actinomycotic mycetoma responds more favorably to treatment than mycetoma caused by a true fungus.[2] If diagnosed sufficiently early, complete excision of a small circumscribed lesion may result in complete cure. Larger lesions require surgical debridement of necrotic and grossly infected tissue plus long-term systemic therapy with ketoconazole or itraconazole.[2] Amputation should be considered as a final measure in large lesions that do not respond to conservative surgical intervention and medical treatment.[1] In our patient, there were no sinuses or granules to suggest that the lesion was mycetoma. This was an unusual presentation of mycetoma. Hay et al. had also reported patients who had longstanding mycetomas without sinuses.[3] We conclude that in endemic areas, mycetoma should be considered in the differential diagnosis of chronic subcutaneous lesions, even if there are no sinuses or discharging grains, as surgical excision of such lesions may result in complete cure. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06043f2.jpg] [dv06043f1.jpg] |
| |||||||||

{kind=link}
{kind=link}