 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
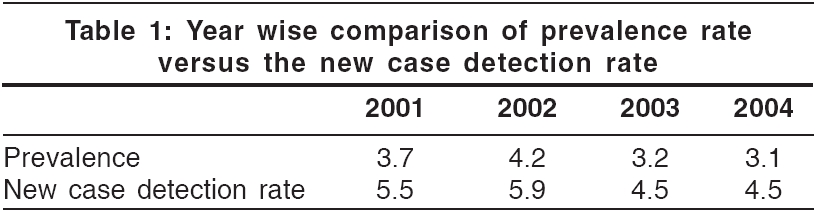
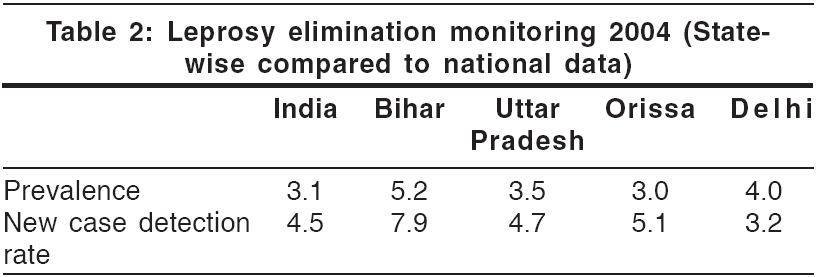
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 151-153 Letter To Editor Final push of leprosy: It is prudent to pause before declaration! Khaitan BinodK, Tejasvi T, Aggarwal Komal, Khanna Neena Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi Code Number: dv06047 Related articles: dv06048 , dv05079 Sir, This is in reference to the article ′Final push of leprosy in India: what is being pushed?′ published in IJDVL.[1] We support the views of Rao and Lakshmi regarding the fallacies of the final-push strategy for elimination of leprosy. ′ Final push′ as a strategy was initiated by WHO in November 1999 with an objective to achieve the target of prevalence rate < 1/10,000 by 2005. Though the prevalence of leprosy is decreasing, we should acknowledge the fact that operational aspects of the program also affect these figures. For example, reducing the duration of treatment by half for patients receiving MB-MDT from 24 to 12 months in effect reduces the prevalence rate by half for that group. Some patients receiving single-dose ROM (rifampicin, ofloxacin and minocycline) treatment for single skin lesion do not appear in prevalence figures at all. Similarly, patients who receive their 6-month course of PB-MDT early in the calendar year also do not figure in the data since only those patients who are on active treatment on 31st December are counted for that year′s prevalence figures. This picture changes when new case detection rates are considered instead of prevalence (the new case detection rate is a better indicator of disease because it is not affected by changing the case definitions or duration of treatment).[2],[3] Though the prevalence has fallen, the new case detection rate has not changed much [Table - 1][Table - 2]. Even at the leprosy clinic at the All India Institute Medical Sciences, New Delhi, a tertiary care hospital, we have registered 230 MB and 62 PB new cases in the last one year (January to December 2005). The whole idea of elimination was based on the hypothesis that at a prevalence of < 1 case per 10,000 population, the transmission of leprosy in the community would be interrupted or would be epidemiologically insignificant. But the high new case detection rates, the proportion of cases treated with MB-MDT (38.3% in 2004 according to leprosy elimination monitoring groups)[4] and the high rates among children (14.7% in 2004 according to leprosy elimination monitoring groups)[4] indicate that leprosy continues to be transmitted in the community. In spite of all the measures taken, the number of new cases being detected is significantly high. Hence, in an effort to reach the elimination target soon, new instructions are given to field staff, the so-called ′Kathmandu recommendations.′ These instructions, such as the order to stop the search for new cases, cannot be justified as the whole program of leprosy elimination is based on the detection and cure of new cases. Not only this, unofficial instructions like ′Do not register single lesion cases for now′ are creating a false impression of the status of leprosy in India. Leprosy workers are being replaced by multipurpose/basic health workers. Other areas of health are being given priority over leprosy. Instead of being intensified, the leprosy program has slowed down and is being diluted. There is an undue hurry to reach elimination targets and corners are being cut. Shortage of staff, absence of active surveillance and false reporting by statistical jugglery (e.g., not incorporating cases being started on treatment and released from treatment in the same calendar year) can lead to failure of the leprosy program. We strongly feel that the authorities that plan, fund and execute the leprosy program should realize that hiding the actual number of leprosy cases will do no good. The ground reality is not going to change. There is a strong need to continue using LEC approaches and active surveillance. We endorse the recommendations of the Global Alliance for Elimination of Leprosy (GAEL) evaluators that the WHO should make it clear that there are still new cases of leprosy, that a range of leprosy activities still needs to be carried out,[3] and that the governments of all affected countries need to be accountable. We also support the recommendation that the World Health Assembly should pass a resolution that addresses leprosy activities beyond 2005. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06047t2.jpg] [dv06047t1.jpg] |
| |||||||||

{kind=link}
{kind=link}