 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
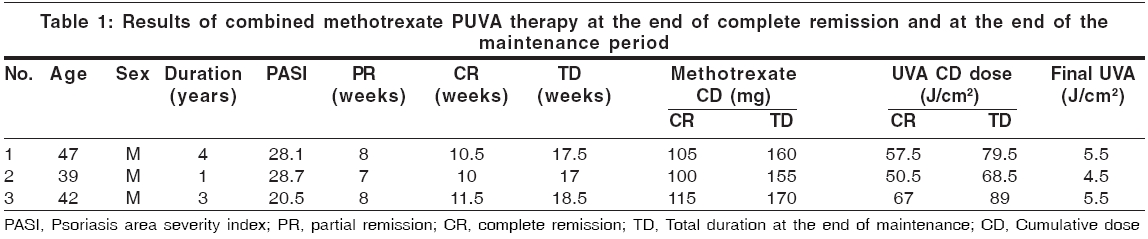
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 153-155 Letter To Editor Modified combined methotrexate PUVA therapy in the treatment of recalcitrant psoriasis: A preliminary report Laxmisha C, P Vinod Kumar, Thappa DM Department of Dermatology and Sexually Transmitted Diseases, Jawaharlal Institute of Medical Education and Research (JIPMER), Pondicherry Code Number: dv06049 Sir, Methotrexate probably reduces the thickness and scaliness of psoriatic plaques, altering the photo-optical properties of the diseased skin so as to increase the penetration of UVA radiation, resulting in the marked reduction in the total cumulative exposure to UVA radiation necessary to achieve remission.[1],[2] Thus, the main advantage of using a combination of methotrexate and PUVA therapy is the marked reduction achieved in the total cumulative exposure to UVA radiation necessary to achieve remission.[1] This was the basis of our trial of this combination therapy on three cases of recalcitrant psoriasis. Three male adults of Fitzpatrick skin type V with recalcitrant psoriasis with a minimum PASI score of 20 (on various topical and systemic treatments) were recruited between December 2003 and March 2005 and those with contraindications for PUVA and methotrexate and on active systemic therapy in the past 8 weeks were excluded. Informed consent was taken from all the patients and the protocol had the approval of the institutional ethical committee. All patients were investigated and followed up as per guidelines for methotrexate usage and PUVA therapy. Complete remission was defined as ′greater than 90% reduction in PASI from baseline′ and partial remission as ′more than 75% reduction from the baseline′. Relapse was defined as ′a PASI score that is 50% more as compared to the baseline′. These patients were started on tablet methotrexate 10 mg/week for a period of 4 weeks. PUVA therapy using 8-methoxypsoralen crystalline tablets at a dose of 0.6 mg/kg body weight was instituted twice a week from week 5 onwards along with the same dose of methotrexate. UVA radiation was delivered with a Dermalight 6000® model (from Dr. Honle, Munchen, Germany) chamber having an irradiance of 14 mw/cm 2 with a starting dose of 3 J/cm 2. The UVA dose was incremented by 0.5 J/cm 2 every second or third sitting depending on the patient′s response to therapy. Once complete remission had occurred, the patient was put on a maintenance dose of PUVA (last clearance dose administered once a week for a period of 4 weeks) along with methotrexate. On completion of the maintenance dose of PUVA, methotrexate was tapered by 2.5 mg every week. The patients were then followed up monthly for a minimum period of 3 months. Partial remission was achieved in all the cases by 7.6 weeks and complete remission by 10.6 weeks. At the time of complete remission, the total number of UVA exposures was 13.3 per person, the mean UVA cumulative dose was 58.3 J/cm 2, the final clearance dose of UVA was 5.16 J/cm 2sub and the mean cumulative dose of methotrexate was 106.6 mg [Table - 1]. Monthly follow-up after the end of the maintenance period of 3 months did not see any relapse. The only adverse events noticed were nausea in two patients and mild pruritus in three patients. The mean cumulative dose of methotrexate and maximal UVA doses in our report were similar to the study by Morison et al .[2] In the present report, the number of PUVA exposures and clearance times were much higher, which could be on account of our cases being recalcitrant in nature, belonging to skin type V, being on lower initial doses of methotrexate, with slow increment in UVA doses and twice weekly PUVA administration and consequently, had no instance of acute or subacute phototoxicity (in comparison to Morison et al .[2] study). Shehzad et al .,[3] utilizing the combination of methotrexate and PUVA therapy, observed that the mean number of PUVA sessions needed for clearance was 10 and the mean time was 2.5 weeks. PUVA administered four times a week may have allowed for faster clearance times in the above studies. Twice-weekly PUVA treatment used by us for psoriasis was proved to be as effective as treatment given more frequently and probably more safe.[4]} References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06049t1.jpg] |
| |||||||||

{kind=link}