 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
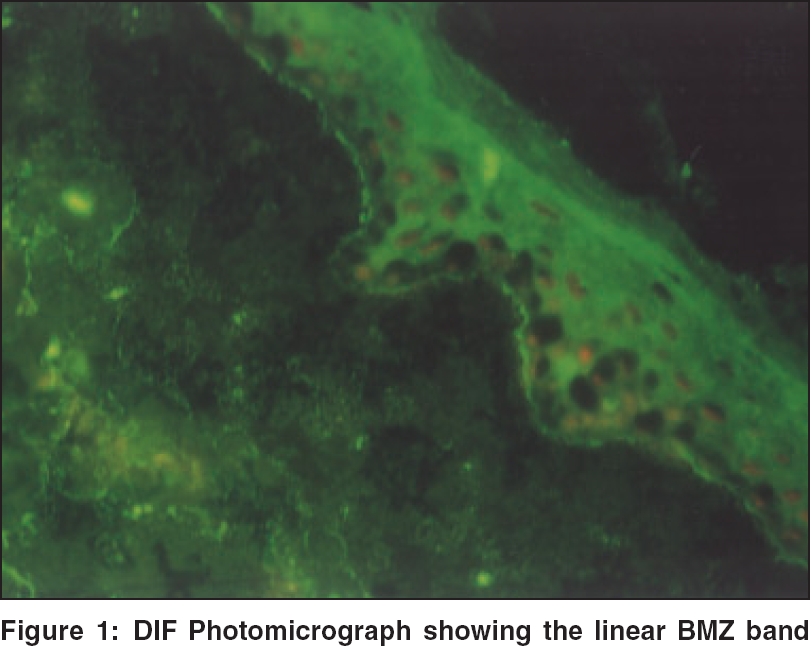
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 158-159 Letter To Editor Localised bullous pemphigoid in the breast Balachandran C, Rai VandanaMehta Department of Skin and STD, Kasturba Medical College and Hospital, Manipal, Karnataka Code Number: dv06052 Sir, A 20-year-old woman presented with recurrent vesiculobullous lesions associated with itching, oozing and crusting around the right areola of 1 year′s duration. The lesions used to subside temporarily with topical steroids and oral antibiotics. On examination, there were vesicles and bullae with crusting and erosions around the right areola. No other areas were involved. There were no oral or genital lesions. Systemic examination was normal. The clinical diagnosis of localized bullous pemphigoid (BP) was confirmed by direct immunofluorescence study of perilesional skin, which showed linear IgG and C3 deposits at the basal membrane level [Figure - 1]. Histopathological examination of a biopsy revealed a subepidermal blister. Indirect immunofluorescence with salt split skin examination and immunomapping is required to confirm the diagnosis and exclude the possibility of localized trauma-induced epidermolysis bullosa acquisita.[1] This was not performed in our patient as she improved dramatically with dapsone 100 mg orally daily and a topical clobetasol propionate-gentamicin combination; the rapid response to treatment makes the diagnosis of epidermolysis bullosa acquisita in our patient unlikely, as this disease does not usually respond well to treatment. Dapsone 100 mg daily was continued for 6 months. There was no relapse on follow-up after another six months. Localized BP is infrequent, but has been documented following radiotherapy, in surgical wounds, secondary to trauma or burns and peristomal lesions.[2],[3],[4] Localized BP affecting the pretibial, oral or vulvar region has also been described,[5] but its pathogenesis is not clear. Some authors consider it the result of different forms of epidermal damage (Koebners phenomenon) in predisposed patients, with the induction of antigen exposure in the context of subclinical pemphigoid followed by activation of the corresponding autoimmune process.[6] While localized BP of the breast after, for example, radiotherapy has frequently been described,[7] we could not find any trigger in our patient. Potent topical corticosteroids are very useful in the treatment of localized BP. The addition of dapsone along with a small dose of oral steroids may be also helpful in patients with recalcitrant disease. Our patient responded well to treatment with oral dapsone and a topical steroid-antibiotic combination. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06052f1.jpg] |
| |||||||||

{kind=link}