 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
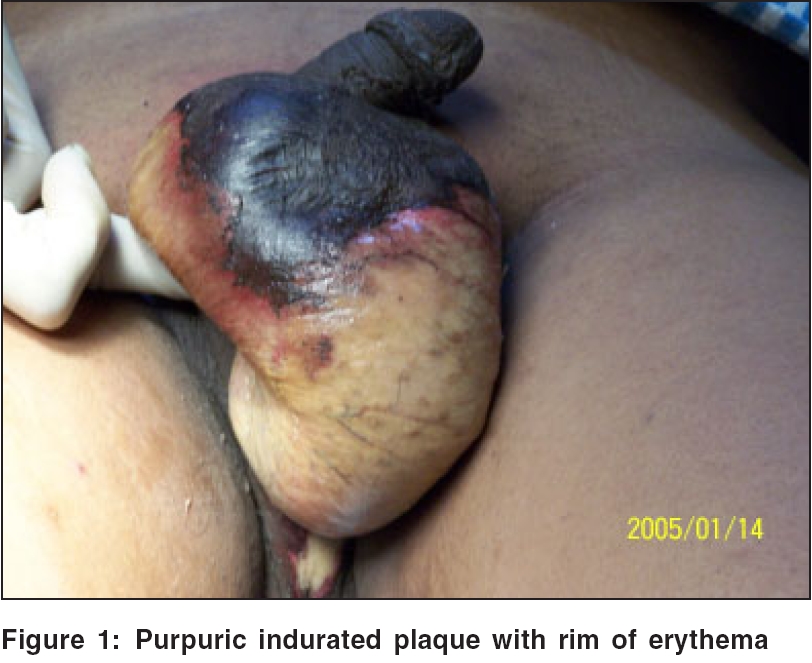
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 159-160 Letter To Editor Split-thickness skin grafting: A novel approach in the treatment of Fournier's gangrene Nikhare SN, Kura MM* Department of Dermatology, Central Railway Hospital, Kalyan, *Grant Medical College, Sir JJ Hospital, Byculla, Mumbai, Maharashtra, India. Code Number: dv06053 Sir, Fournier′s gangrene is an uncommon rapidly progressive polymicrobial (aerobes and anaerobes) infection of the genital, perineal and perianal region,[1],[2],[3],[4] resulting in necrotizing fasciitis, due to endarteritis of scrotal vessels and gangrene of the scrotum.[1] It can involve contiguous areas like the lower urinary tract, anus, rectum and colon. The course of disease is rapid and the disease can be lethal if not treated urgently. Fournier′s gangrene is more common in males and can present in any age group. Predisposing factors are diabetes, alcoholism, old age, HIV infection and malnutrition.[1],[2],[3],[4],[5],[6] Operative procedures like vasectomy, circumcision, hysterectomy, pudendal nerve block and episiotomy may also lead to Fournier′s gangrene.[1] It has also been reported following insect bite and trauma in children.[1],[4] The diagnosis is mainly clinical.[1] Treatment involves debridement and intravenous administration of broad-spectrum antibiotics.[4],[5],[6],[7],[8] Even with aggressive surgical debridement, the mortality rate ranges from 8 to 67%.[1] Reconstruction of the scrotum and perineal area can be done after the infection is controlled. Orchidectomy and/or penectomy may be required.[8] Methods for reconstruction of the scrotum include burying the testes in the thigh or in the abdomen;[1] split-thickness skin grafting (STSG) with mesh technique, a technically easy and safe method with satisfactory results; and wide surgical debridement with secondary suturing.[4],[5],[6] We report successful treatment of a patient of Fournier′s gangrene by reconstruction of the scrotum with split-thickness skin grafting. A 39-year-old male presented with a 2-day history of pain and swelling of the scrotum. On examination, the scrotum showed a diffuse tender swelling and a localized purpuric plaque with a broad rim of erythema [Figure - 1]. Based on the clinical features, a diagnosis of Fournier′s gangrene was made. The hemogram and blood sugar levels were normal. The HIV (ELISA) test was negative and the VDRL test was nonreactive. He was hospitalized and treated by wide excision and debridement [Figure - 2]. After a week, the denuded area was covered with healthy granulation tissue. Considering the large ulcer area, split-thickness skin grafting was done. The grafts were well taken in 80% of the area. The patient was put on injection cefotaxime 1 g TID intramuscularly, injection gentamycin 80 mg BD intravenously and metronidazole 400 mg TID orally for 10 days. The donor area healed up completely in 2 weeks. By 35 days the grafts completely covered the ulcer and by 6 months the scrotal skin had a near-normal appearance [Figure - 3]. Fournier′s gangrene is a rapidly progressive necrotic disease of the genital region that may be potentially lethal. It needs prompt surgical intervention and parenteral antibiotic therapy. Hyperbaric oxygen therapy has also been advocated. After the phase of acute necrosis and debridement, treatment of the wide areas of denuded skin in the genital, perineum and perianal region is a difficult task. Since healing with secondary intention may take a very long time, reconstructive surgery may be needed. Split-thickness skin grafting (STSG) is a safe and easy method to cover these raw areas. However, stabilizing the grafts may be difficult due to free mobility of the testicles. STSG can be done by using stamp-sized grafts or by the mesh technique. Mesh skin grafting offers the advantage of covering a large area with a small sheet of donor skin but needs specialized equipment, i.e., mesh graft plate and roller. In our patient, we used stamp sized multiple skin grafts to achieve maximum coverage of the denuded area of the perineum and scrotum. As reconstructive surgery is rarely performed by dermatologists, Fournier′s gangrene is rarely managed by dermatologists. However, as in this patient, split-thickness skin grafting was done by a dermatosurgeon with excellent results. Acknowledgment The authors thank all the consultants of Central Railway Hospital, Kalyan, who contributed to the study and provided care to the patient. The authors also thank Dr. Santosh Daflapurkar, Mrs. Jagruti Nikhare and Mr. Bhavikatti for their assistance.References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06053f1.jpg] [dv06053f3.jpg] [dv06053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}