 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
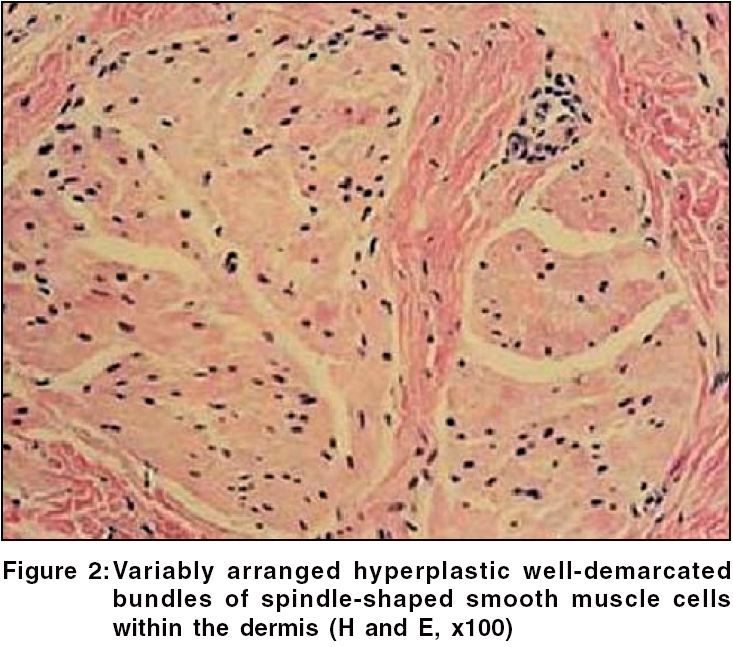
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 2, March-April, 2006, pp. 178 Net Case Acquired smooth muscle hamartoma Bari Arfan ul, Rahman Simeen Ber* Combined Military Hospital, Azad Jammu Kashmir, Pakistan; *Department of Dermatology, Military Hospital, Rawalpindi, Pakistan. Code Number: dv06059 Abstract Smooth muscle hamartoma is an uncommon, usually congenital, cutaneous hyperplasia of the arrectores pilorum muscles. When it is acquired, it may be confused with Becker's nevus. We report a case of this rare tumor in a 19-year-old man. The disease started several years ago as multiple small skin-colored papules that subsequently coalesced to form a large soft plaque on the back of the left shoulder. The diagnosis of acquired smooth muscle hamartoma was confirmed on histopathology. The patient was reassured about the benign nature of the lesion and was not advised any treatment.Keywords: Becker′s nevus, Smooth muscle cutaneous tumors, Smooth muscle hamartoma A smooth muscle hamartoma is a rare benign proliferation of smooth muscle, first described by Stokes in 1923.[1] Initially, it was known as congenital smooth muscle neoplasm but later, a few cases of the acquired variant were also described. When it is acquired, it may be confused with Becker′s nevus, with a prominent smooth muscle component. Both entities can be considered polar forms of a spectrum of dermal smooth muscle hyperplasia. Here, we describe a case of acquired smooth muscle hamartoma that simulated Becker′s nevus. Case History A 19-year-old, otherwise healthy, man presented with an asymptomatic large reddish-brown plaque on a circumscribed area of the left shoulder. He complained of occasional itching in the lesion but no discomfort or pain. There was no history of similar lesions in the family. It started as multiple small papules about 7 years ago, which gradually grouped together and coalesced to reach the present size. On examination, the patient had a large indurated plaque with an irregular surface, speckled pigmentation, clearly defined margins but with no hypertrichosis [Figure - 1]. The pseudo-Darier sign was weakly positive. His routine laboratory investigations were within normal limits. Results of biopsy specimens showed an excess of haphazardly oriented smooth muscle bundles in the mid- to lower dermis with an unremarkable overlying epidermis [Figure - 2], thus confirming a diagnosis of acquired smooth muscle hamartoma. Considering the asymptomatic benign nature of the neoplasm and the almost no risk of malignant change, he was reassured. No surgery was adviced as the site was not of high cosmetic importance. Discussion Congenital smooth muscle hamartoma is usually characterized by frequent prominence of vellus hairs; darker, longer, or thicker hair; and variable hyperpigmentation and epidermal change. The degree of hypertrichosis, pigmentation and induration may change with time. The lesions usually occur on the trunk and proximal extremities and present more frequently in male patients. Patches, plaques, or less frequently papular follicular lesions may be noted. Transient piloerection or elevation of a lesion induced by rubbing, referred to as a pseudo-Darier sign, is often seen.[2],[3],[4],[5] Interestingly, cutaneous smooth muscle hamartomas are said to be the underlying lesions in the ′Michelin tire baby′syndrome in boys.[6] Ordinary congenital smooth muscle hamartomas have shown no evidence of malignant transformation and do not appear to be associated with other congenital abnormalities.[2] Rarely, smooth muscle hamartomas occur as acquired lesions without hyperpigmentation or hypertrichosis and these acquired cases have been reported to occur on the abdomen, shoulder, vulva, penis and scrotum.[2],[7],[8],[9],[10] Histopathologically, congenital smooth muscle hamartoma comprises variably oriented, discrete, hyperplastic smooth muscle bundles within the reticular dermis. Variable acanthosis and hypermelanosis may be seen. Histochemical stains such as Masson′s trichrome and phosphotungstic acid-hematoxylin or immunohistochemical stains may illustrate the smooth muscle nature of the proliferation. Electron microscopic evaluation demonstrates myofilaments, continuous basal lamina, dense bodies, pinocytotic vesicles and nerve fibers.[2],[3],[4],[5] The clinical differential diagnosis for congenital smooth muscle hamartoma includes a solitary mastocytoma, café au lait spot, congenital pigmented hairy nevocellular nevus, Becker′s nevus and myokymia. These lesions are not indurated and do not exhibit a positive pseudo-Darier sign. Hypertrichosis is not seen in a café au lait spot or a mastocytoma. Becker′s nevus may be differentiated by clinical history or electron microscopic studies. Myokymia is characterized by spontaneous, often asymptomatic, undulations of muscle fibers of variable duration.[2],[3],[4],[5] Treatment of smooth muscle hamartomas is not necessary but involves surgical excision if desired.[2] Despite similar histologic findings, controversy exists as to whether smooth muscle hamartoma is a distinct clinicopathologic entity or a form of Becker′s nevus. Becker′s nevi are usually located on the shoulder of adolescent males with hyperpigmentation, hypertrichosis and frequently, proliferation of smooth muscle.[2],[3],[4],[5] In addition, dermal random smooth muscle proliferation with hypermelanosis and acanthosis has been reported as being a possible congenital Becker′s nevus. It is now proposed that these lesions are perhaps best considered as a spectrum. At one end is congenital smooth muscle hamartoma with congenital onset that may occur in the absence of epidermal changes or clinical pigmentation and at the other end, Becker′s nevi, which usually have a childhood or adolescent onset, hyperpigmentation and hypertrichosis. Further support for this proposal is given by some studies that report an abnormal whorled myofilament pattern in electron microscopic studies of congenital smooth muscle hamartoma, which is not seen in Becker′s nevus smooth muscle proliferation.[2],[4],[5] However, both conditions have also been reported to occur together in the same patient.[11] Smooth muscle hamartomas occurring as acquired lesions without hyperpigmentation or hypertrichosis have been rarely described and our patient is an addition to those few reports. It appeared in adolescence like an acquired Becker′s nevus but did not contain hypertrichosis or marked hyperpigmentation. The pseudo-Darier sign was also not strongly positive in our patient as it is likely to diminish in intensity with age and even may be negative. It is believed that the pseudo-Darier sign may be produced by the prominent nerve fibers observed between smooth muscle bundles under electron microscopy, in contrast to the histamine-induced urticarial Darier sign, associated with urticaria pigmentosa.[2],[5] References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06059f1.jpg] [dv06059f2.jpg] |
| |||||||||

{kind=link}
{kind=link}