 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
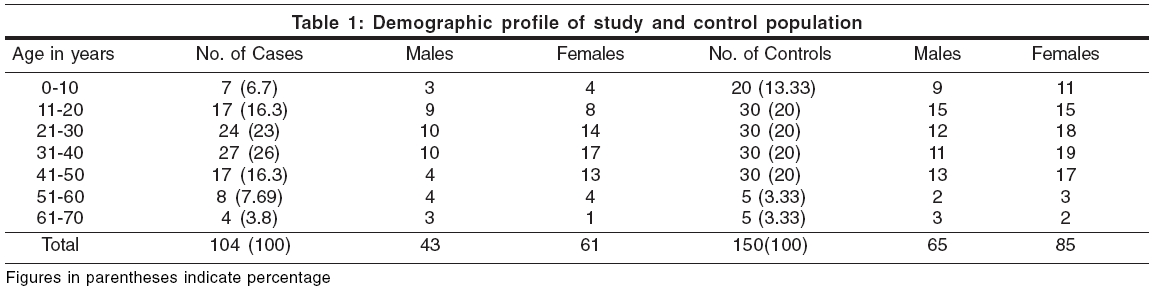
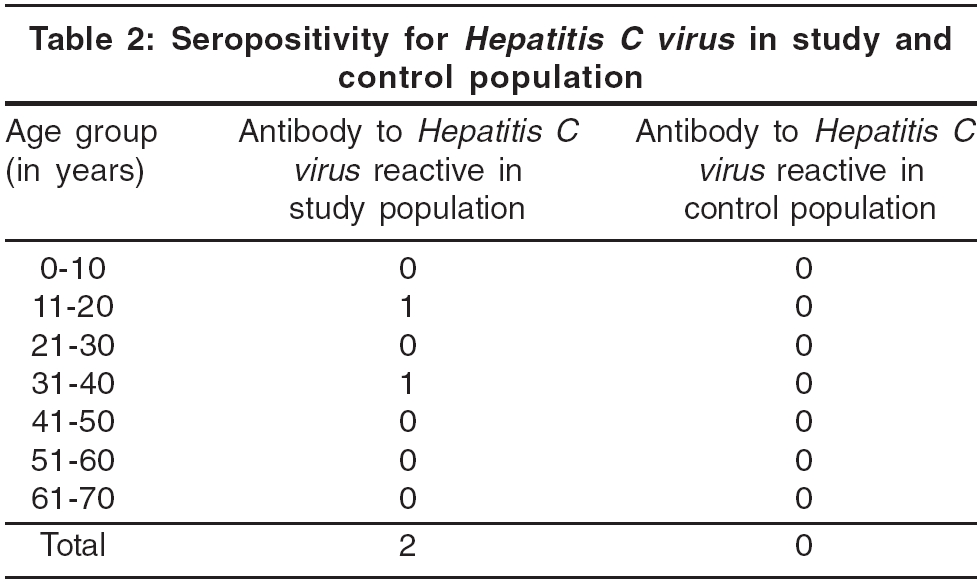
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 3, May-June, 2006, pp. 198-200 Original Article No association between seropositivity for Hepatitis C virus and lichen planus: A case control study Das Arup, Das Jayasri, Majumdar Gautam, Bhattacharya Nandita, Neogi DhrubaKumar, Saha Bibhuti Departments of Pathology, School of Tropical Medicine, Kolkata Code Number: dv06066 Abstract Background: The epidemiological association of lichen planus (LP) with hepatitis C virus (HCV) infection has been recorded from some countries and HCV RNA3 has been isolated from lesional skin in patients with LP and chronic HCV infection. The observed geographical differences regarding HCV infection and LP could be immuno-genetically related. Keywords: Lichen planus, Hepatitis C Virus Introduction Lichen planus (LP) is thought to be an immunologically mediated disorder. In LP lesions, there is infiltration in the dermis of T cells, both CD4+ and CD8+ , while CD8+ T cells infiltrate the epidermis. The CD8+ cytotoxic T cells recognize an unknown antigen associated with major histocompatibility complex (MHC) class I on lesional keratinocytes and lyse them.[1],[2] A genetic susceptibility to idiopathic LP has been proposed. A familial incidence of 10.7% was quoted in one study.[3] An epidemiological association of LP with hepatitis C virus (HCV) infection has been recorded, especially in patients from Italy, where immunogenetic factors such as HLA-DR6 allele may account for geographical differences with regard to HCV infections and LP, and from certain parts of France, Italy, Spain, Japan and Pakistan.[4],[5] Some workers have isolated HCV RNA from lesional skin in patients with LP and chronic HCV infection[6],[7] and an HCV related product has been postulated as a possible antigen in LP. However, patients from northern Europe (including the UK), USA and Nepal have shown no association between LP and HCV infection.[8],[9],[10],[11] We conducted this study to determine whether HCV has a causal relationship with LP in Indian patients. Methods This study was conducted in the Department of Dermatology and Leprology of the School of Tropical Medicine, Kolkata, from patients attending our hospital. The hospital caters to many patients from the eastern parts of India, and from Nepal and Bangladesh. Patients clinically diagnosed as LP between May 2004 and May 2005 were biopsied. All biopsy proven cases of LP were screened for HIV-1 and 2 because HIV infection may interfere with interpretation of HCV seropositivity. However, none were detected seropositive. The HIV-seronegative patients were tested for antibody to HCV by the reagent kit, SP-NANBASE C-96 3.0, developed by the General Biologicals Corporation, Taiwan ROC which adopts the second antibody "sandwich principle" as the basis for the assay to detect antibodies to HCV. This third generation anti-HCV diagnostic kit features structural and non-structural antigens specific for HCV. The results were analyzed and compared with those of 150 HIV-seronegative controls selected from the out-patient department not suffering from LP and who were ready to participate in the study. These controls were more or less matched for age and sex [Table - 1]. There were 104 patients studied [Table - 1], 43 (41.3%) males and 61 (58.7%) females. The male to female ratio was 1:1.41. The maximum number of patients (26 %) was in the 31-40 years age group. Two patients, both male, aged 18 years and 40 years were reactive to antibody to HCV, while all 150 age and sex matched controls were HIV-1 and -2 negative and also negative for antibody to HCV [Table - 2]. Two was too insignificant a number to apply any statistical methods, e.g. Chi square test or Fisher′s exact test etc. Discussion HCV infection has been proposed as a factor in the pathogenesis of LP. Depending on the background rate of HCV infection in the region, 4% to 38% of LP patients may have co-existing HCV infection.[12] In Northern Japan, where the seroprevalence of HCV infection is 8%, 60% of patients with oral LP had HCV infection.[12] One group had reported that 5% of all HCV infected patients have LP.[1] An epidemiological association of LP with HCV infection has been recorded in patients from various parts of the world and HCV RNA has been isolated from lesional skin in patients with LP and chronic HCV infection.[2],[10] Thus, an HCV related product has been postulated as a possible antigen in LP. It has been suggested that the observed geographical differences with regard to HCV infection and LP could be related to immunogenetic factors, such as the HLA-DR 6 allele, which is significantly expressed in Italian patients with oral LP and HCV infection.[4] However, no association between LP and HCV infection has been noted in patients from Northern Europe (including the UK), USA and Nepal.[11],[12],[13],[14] We tested 104 patients of biopsy proven LP who were HIV-seronegative for antibody to HCV. Only two patients suffering from generalized LP of more than 3 months′ duration were anti-HCV antibody positive. The background rate of seroprevalence of HCV as per unpublished data of our virology department is 0.8%. All 150 controls of comparative age and sex groups tested negative for anti-HCV antibody. We did not find any significant association between LP and HCV. In fact, the number of HCV positive patients was so low that we could not apply any statistical methods. Our results are comparable with other Indian studies[14],[15],[16] where only 2.66% cases were positive for the HCV antibody, which is almost parallel to the prevalence of HCV in the general population in India (1.5 to 2.2%).[3] However, while studies conducted in New Delhi have failed to demonstrate statistically significant association between HCV and LP,[17] studies conducted in Hyderabad and Bangalore have shown a significant association.[4],[5] Whether the geographical variation of Hep C seropositivity prevalence among LP patients may be attributed to genetic factors remains to be studied. All the previously done studies including the present study suffer from the shortcoming of inadequate sample size. Future studies should be large enough to take into account this requirement and settle this issue. Acknowledgements We acknowledge the contribution by Dr Sreema Adhikari, Virology Department, for most of the tests of the virology portion of this study and by Shri Tapan Kumar Kar, Medical Technologist, Virology Department, School of Tropical Medicine, for his technical assistance in anti-HCV tests.References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06066t2.jpg] [dv06066t1.jpg] |
| |||||||||

{kind=link}
{kind=link}