 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
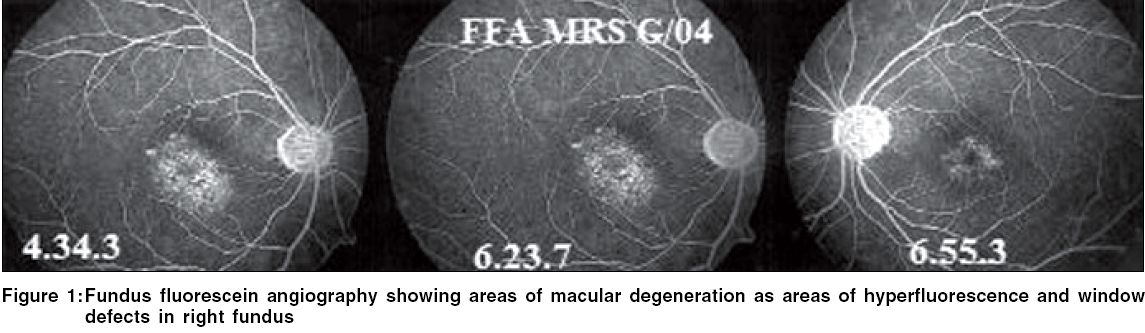
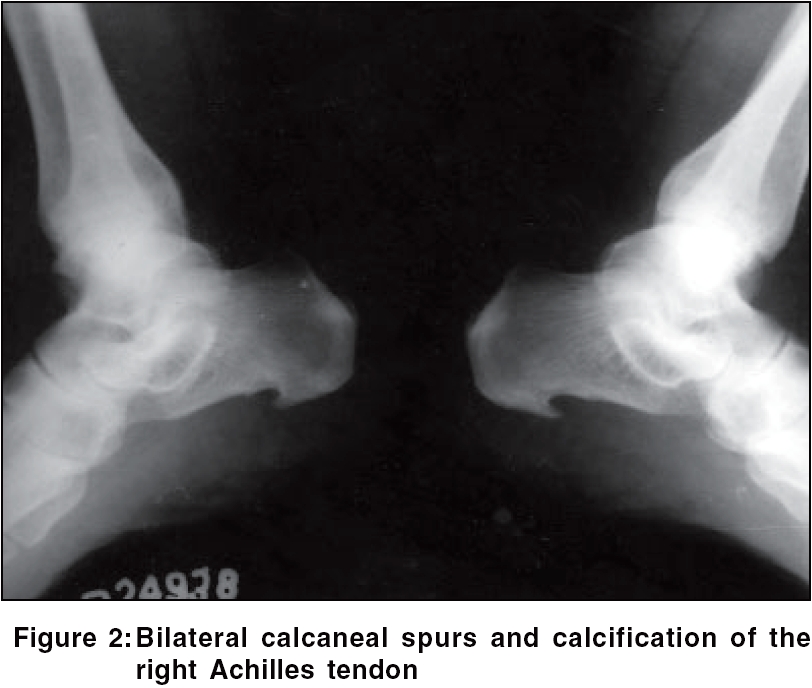
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 3, May-June, 2006, pp. 227-230 Case Report Macular degeneration in a case of Reiter's disease Sawhney MPS, Parihar JKS Department of Dermatology and STD, Base Hospital, Barrackpore Code Number: dv06075 Abstract Posterior uveitis is not a documented feature of Reiter's disease. We describe here a patient of Reiter's disease, who after a bout of dysentery in January 2002 developed macular edema of the right eye with visual acuity of 6/36. In December 2002, she was found to have phlyctenular conjunctivitis. In June 2004, when she reported with scaly plaques over both palms, repeat ophthalmological examination revealed macular degeneration of the right eye. The simultaneous occurrence of Reiter's disease and macular degeneration in this patient may be fortuitous but the immunological basis of both diseases suggests a possible association. Keywords: Macular degeneration, Phlyctenular conjunctivitis, Posterior uveitis, Reiter's disease Introduction In 1916, Hans Reiter described Reiter's disease as a clinical triad of urethritis, conjunctivitis and polyarthritis.[1] Conjunctivitis of varying intensity that usually resolves quickly is the predominant lesion of the disease.[1],[2],[3] Severe iritis or keratitis may also be associated and recurrent attacks of iridocyclitis may lead to blindness.[1],[2] The uveitis resembles that of ankylosing spondylitis in that it is acute in onset, frequently unilateral and spares the choroid and retina.[2],[3] We report a case of Reiter's disease with macular degeneration of the right eye.Case report A 51-year-old female reported to the Dermatology outpatient department in June 2004 with complaints of scaly plaques over both palms since one and a half years. On enquiry, she gave a history of pain in both heels, for which she was diagnosed as a case of plantar fasciitis in 1984, treated with intralesional corticosteroid and improved. She was diagnosed as a case of idiopathic hypothyroidism in 1989 and was on thyroxin replacement therapy since then. She developed primary hypertension in 1991. She also gave a history of copious, thin, non-foul-smelling vaginal discharge with congestive dysmenorrhea, menorrhagia and irregular periods since 1994. When this did not improve with dilatation and curettage (done thrice), she underwent hysterectomy in 1997. In 1998, she had an attack of cervical spondylitis, for which she was treated symptomatically. In January 2002, she had a bout of dysentery along with fever lasting for 25 days, which was accompanied by sudden visual impairment in the right eye. Admitted to a military hospital in Delhi, she was found to have vision of 6/60 in the right eye. Fundus examination revealed macular edema, which was managed with systemic steroidal and nonsteroidal anti-inflammatory drugs, after ruling out tuberculosis. Repeat ophthalmic examination on 7th December 2002 had revealed phlyctenulosis of both eyes, which improved with the use of corticosteroid eye drops. Fundus examination had revealed resolved macular edema with residual hyperpigmentation in the parafoveal region. She was found to have hepatomegaly while being investigated for arthritis and was treated with tinidazole and doxycycline for 10 days by a physician in August 2002. She gave a history of arthritis of both knees, for which she had been investigated for connective tissue disorders; the ANA, rheumatoid factor, LE cell phenomenon and cryoglobulins were all found negative and the serum uric acid was normal. The patient's husband was diagnosed as a case of Reiter's disease in June 2004. General and systemic examinations were normal. She had swelling and tenderness of both knee joints with normal mobility. Dermatological examination revealed scaly plaques over both palms with copious silvery scales. The nail, hair and mucosae were normal. Ophthalmological examination revealed normal anterior segment, including the lens, of both eyes. Her best-corrected visual acuity was 6/6 in the left eye and 6/36 in the right eye. Fundus examination of the left eye revealed stippling and hyperpigmentation in the macular region and surrounding parafoveal area. The changes in the right fundus (dull foveal reflex, areas of hyperpigmentation and hypopigmentation as well as multiple drusen and a few hard exudates involving the posterior pole) were highly suggestive of post-inflammatory macular degeneration. These findings were confirmed by fundus fluorescein angiography as areas of hyperfluorescence and window defects [Figure - 1]. The patient's hemogram, urine examination, blood urea, serum creatinine, liver function tests, blood sugar (fasting and postprandial) and radiograph of the chest were normal. HLA-B27 was positive. Radiographs revealed bilateral large calcaneal spurs and calcification of the right Achilles tendon [Figure - 2]; syndesmophytes over C4, C5 and C6 vertebrae [Figure - 3] and osteophytes over both tibia and femora. She was diagnosed as a case of Reiter's disease with macular degeneration of the right eye. She was treated with a two-week course of doxycycline and then started on methotrexate therapy 7.5 mg/week in three equal 12-hourly divided doses since 5th June 2004 and gradually increased to l5 mg/week. Arthritis of the knee, spondylitis and heel pain improved after 3 months. The scaly plaques over the palms regressed completely, but a few lesions reappeared after 3 months and she was given another course of an anti-chlamydial drug, erythromycin. There was considerable improvement in joint pains and scaly plaques at the end of 4 months. Repeat ophthalmological examination revealed no change. Discussion The association of HLA-B27 with seronegative spondyloarthropathies like Reiter's syndrome, psoriatic spondylitis and the spondylitis of inflammatory bowel disease is one of the best examples of a disease association with a hereditary marker.[4],[5] The risk of Reiter's disease development in HLA-B27 carriers is 27 times higher than the mean incidence of this disease in the population.[6],[7] The incidence of anterior uveitis in Reiter's syndrome is significantly higher with HLA-A9 and -B40 antigen combinations as compared to -A1 and -B27.[6],[7] Evidence of enthesopathy in the form of plantar fasciitis, calcaneal spur, enthesopathy involving other weight bearing joints and spine in the presence of symptoms of genitourinary infection is diagnostic of Reiter's disease. Phlyctenular conjunctivitis is a delayed hypersensitivity response to microbial proteins. It has been described in Chlamydia trachomatis infection with serotypes Ll, L2 and L3[3] but not specifically in Reiter's syndrome caused by serotypes D to K, which are responsible for nongonococcal urethritis.[7] Conjunctivitis is one of the components of the triad of this syndrome and phlyctenular conjunctivitis may be another type of conjunctivitis associated with it. Association of phlyctenular conjunctivitis with Reiter's syndrome is speculated here on the basis of common etiological relationship of Reiter's disease and phlyctenular conjunctivitis to Chlamydia trachomatis infection. The anterior segment of the eye may be involved in Reiter's disease, but focal posterior involvement is a rare feature of Reiter's syndrome or the reactive arthritis group.[8] Macular degeneration of the retina may follow inflammatory retinitis. Most cases of posterior uveitis involving the choroid and retina are associated with some form of systemic disease.[2],[3],[8] Our patient developed macular degeneration of sudden onset following a bout of dysentery. The organism responsible for dysentery could have acted as another antigenic trigger in a genetically susceptible host, producing immunologically mediated posterior uveitis with retinal damage.[6],[7],[9] Although the simultaneous occurrence of Reiter's disease and macular degeneration in this case may be fortuitous, the immunological nature of both these illnesses and the sequence of events suggest an association. Only one case of retinal involvement in the form of bilateral detachment has been described earlier.[9] In patients with chronic ocular manifestations of Reiter's syndrome referred to a tertiary ocular centre, anterior uveitis was found in 92%, posterior uveitis in 64%, intermediate uveitis in 40% and cystoid macular edema in 28%.[10] However, none of the patients had macular degeneration. To conclude, while involvement of the anterior segment of the eye in Reiter's disease is well-recognized, focal involvement of the posterior segment with macular degeneration, as seen in our patient, is probably a rare feature of Reiter's syndrome or the reactive arthritis group. Phlyctenular conjunctivitis as seen in our case, though not described earlier with Reiter's disease, has been described in infection with L1, L2, L3 serovars of C. trachomatis and thus may be one another type of conjunctivitis in Reiter's disease. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06075f3.jpg] [dv06075f2.jpg] [dv06075f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}