 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
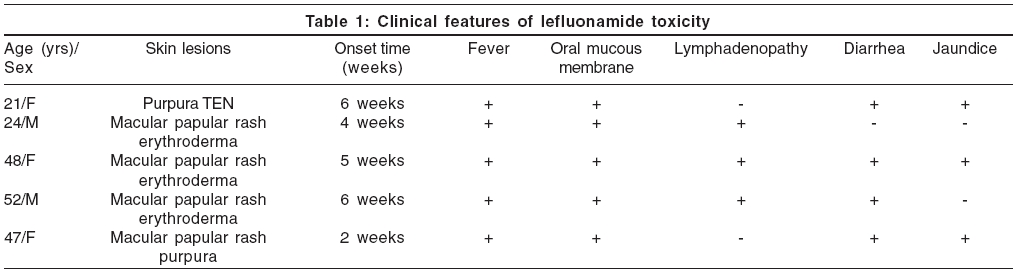
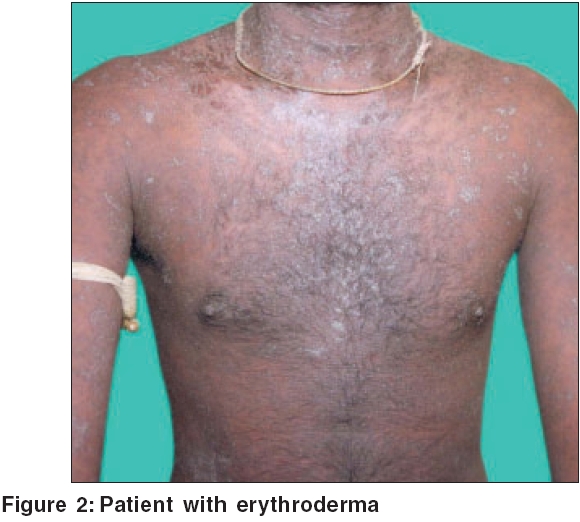
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 4, July-August, 2006, pp. 286-289 Brief Report Severe cutaneous adverse drug reaction to leflunomide: A report of five cases Shastri Veeranna, Betkerur Jyayadev, Kushalappa PA, Savita TG, Parthasarathi G Department of Skin and STD, J. S. S. Medical College Hospital, Ramanuja Road, Mysore - 570 004, Karnataka Code Number: dv06097 Abstract Medications used to treat human ailments are known to cause cutaneous reactions which may vary in their severity. Leflunomide, an immunomodulating agent recently introduced to treat rheumatoid arthritis, is reported to cause severe cutaneous reactions. We are reporting five such cases. All our patients were started on leflunomide for rheumatoid arthritis, 4-6 weeks before the onset of cutaneous reaction and were admitted to the hospital with the common complaints of fever, skin rash and generalized weakness. All of them had characteristic pattern of events such as delayed onset of reaction, widespread and long lasting skin rash and internal organ involvement. These features suggest a possibility of drug hypersensitivity syndrome to leflunomide. Careful dosing and periodic monitoring of patients treated with leflunomide for possible adverse drug reaction is recommended.Keywords: Adverse drug reaction, Leflunomide, Severe cutaneous reactions, Drug hypersensitivity syndrome Introduction Cutaneous adverse drug reactions (CADRs) are the most prominently seen ADRs. The clinical spectrum of CADRs ranges from pruritus to severe life-threatening reactions like erythema multiforme (EM), Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) and drug hypersensitivity syndrome (DHS). Many drugs including ciprofloxacin, carbamazepine, dapsone, isoniazid, clindamycin, diclofenac, rifampicin and zidovudine are known to cause severe cutaneous reactions. Leflunomide is a new immunomodulating agent and disease-modifying antirheumatic drug with anti-inflammatory and immunosuppressive activity, used in the treatment of active rheumatoid arthritis. It has been reported to cause various CADRs including SJS, TEN and EM, in less than 1% of the patient population.[1] We report five cases of severe CADR induced by leflunomide [Table - 1]. Case Reports Case 1 Case 2 Case 3 Case 4 Case 5 Discussion Leflunomide is a new immunomodulatory drug approved by the USFDA in Sept 1998, for the treatment of RA. It inhibits pyrimidine synthesis, resulting in antiproliferative and anti-inflammatory effects. It is a prodrug, which is converted to its active metabolite A771726 with a half-life of two weeks.[1] There are several reports of mild to severe adverse drug reactions associated with leflunomide. The approved/labeled indication for the use of leflunomide is RA.[2],[3] However, it is being recommended for dermatological conditions like psoriatic arthropathy, vasculitis, sarcoidosis and autoimmune bullous diseases.[4] All five patients reported here had taken leflunomide for RA, 2-6 weeks prior to the onset of symptoms. They presented with fever, skin rash and internal organ involvement. Skin lesions started as exanthematous and purpuric rash, which progressed to erythroderma in three cases and TEN in one case. All patients had long lasting skin lesions. Three patients had lymphadenopathy and three had diarrhea. All patients had leukocytosis; one had eosinophilia; two patients had hyperbilirubinemia. Skin biopsy was done in three cases. Histopathology showed vacuolar degeneration of basal cells, exocytosis, focal subepidermal clefting, occasional necrotic keratinocytes and perivascular lymphocytic infiltration. Leflunomide was stopped in all patients. Systemic steroids and other supportive treatment were given. Two patients received oral chloestyramine 4 gm tid. Chloestyramine is expected to help in the excretion of leflunomide by interfering with biliary secretion and reabsorption of leflunomide.[5] Three of the five patients recovered completely, one was lost to follow up, while, one died. We could not ascertain the cause of death, as the patient was shifted to another hospital, where she died. A similar case of leflunomide-induced severe cutaneous reaction with hepatitis and skin rashes with fatal outcome, is reported in Indian literature.[5] All our patients had characteristic pattern of events like delayed onset of reaction, fever, widespread and long lasting skin rash and internal organ involvement. These features suggest a possibility of drug hypersensitivity syndrome (DHS). Other differential diagnosis considered in these cases, were infections such as Epstein Barr virus infection, Kawasaki disease, HIV infection, viral hepatitis, enteric fever, rickettsial infection, graft-versus-host disease, lymphoma and autoimmune connective tissue diseases. We assessed the causality of reported ADRs by adopting two different causality assessment scales viz. World Health Organization's ADR probability scale[6] and Naranjo's scale.[7] Upon assessment of causality by taking all the relevant data into the account, four reactions were found probable and one was possible for leflunomide by both scales. The pathogenesis of DHS is not well understood. These patients show a partially inherited increased susceptibility to the toxic effects of oxidative drug metabolites. These reactive metabolites cause immunological reaction by either forming hapten or by danger signalling. An interaction between drugs and viral infection like HIV has been implicated in the pathogenesis of DHS.[8],[9] The current recommended dosage schedule for leflunomide is 100 mg once daily for 3 days, followed by 20 mg once daily. This initial high dosage may trigger the formation of toxic metabolites, with resultant clinical syndrome of multiorgan dysfunction. The gradually increased dose regimen as in case of nevirapine and lamotrigine, may lead to adaptive changes that reduce the risk of hypersensitivity reaction in susceptible individuals, making this method of drug administration, a form of prophylactic drug desensitization.[10] Five cases of severe adverse drug reaction to leflunomide with clinical manifestations suggesting DHS, are reported. We believe that clinicians should be alerted to the possibility of the severe reactions reported here. Careful dosing and periodic monitoring of patients treated with leflunomide for possible adverse drug reaction is recommended. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06097f2.jpg] [dv06097f1.jpg] [dv06097t2.jpg] [dv06097t1.jpg] [dv06097f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}