 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
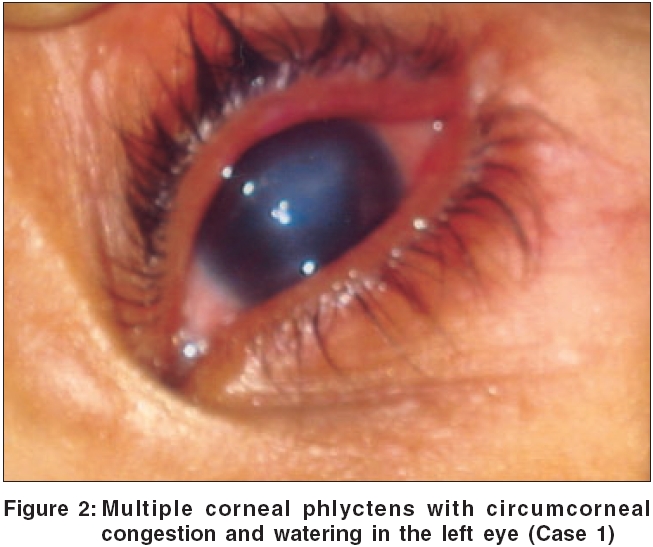
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 4, July-August, 2006, pp. 290-292 Case Report Cutaneous tuberculosis and phlyctenular keratoconjunctivitis: A forgotten association Singal Archana, Aggarwal Puneet, Pandhi Deepika, Rohatgi Jolly Department of Dermatology and STD, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi - 110 095 Code Number: dv06098 Abstract Cutaneous tuberculosis may be associated with concurrent systemic foci in the body such as lung, lymph node, bone or CNS. Phlyctenular keratoconjunctivitis (PKC) is a manifestation of immunological response to a variety of antigens in the eye, tubercular focus (evident or occult) being the commonest in India. Reports in the existing literature have shown lungs and lymph nodes to be the predominant underlying focus associated with PKC, whereas cutaneous tuberculosis has seldom been found in this situation. We report this forgotten association in two children with cutaneous tuberculosis, one each with lupus vulgaris and scrofuloderma, who also had PKC. Interestingly, one of the cases also had simultaneous lichen scrofulosorum, which is also an immunological response to tubercular antigen and manifests in the skin, thus showing immunological manifestation in two different organ systems along with cutaneous focus of tuberculosis.Keywords: Lupus vulgaris, Scrofuloderma, Phlycten, Cell-mediated immunity Introduction Extra-pulmonary tuberculosis constitutes 10% of total tuberculosis and 1.5% of these have cutaneous disease.[1],[2] Phlyctenular keratoconjunctivitis (PKC) represents an allergic cell mediated response in cornea and/or conjunctiva to some antigen, to which they have already become sensitized.[3] In a series from India, tuberculosis accounted for up to 77% cases of PKC.[3] However, only a few published reports documenting the association of cutaneous tuberculosis and PKC exist in the current world literature.[4],[5],[6] The present report highlights this association in two children.Case reports Case 1 Hemogram, liver and kidney function tests were unremarkable. Erythrocyte sedimentation rate was 38 mm in the 1st hour and Mantoux test (1 PPD) was 16 mm after 48 hours. Stool examination revealed no ova or cyst. Bacterial culture from lid margin and conjunctiva was sterile. Fine needle aspiration cytology (FNAC) from the skin lesion and lymph node showed granulomatous infiltrate comprising epithelioid cells and occasional acid fast bacilli (AFB), on Ziehl-Neelsen staining. Skin biopsy revealed epithelioid cell granuloma, Langhans'giant cells and minimal caseation necrosis without AFB in the upper dermis, consistent with lupus vulgaris. Culture for Mycobacterium tuberculosis on Lowenstein Jensen (LJ) and radiometric liquid culture medium BACTEC ® 460 TB System (Becton Dickinson Diagnostic Instrument Systems Sparks, Maryland, USA), did not show any growth. A diagnosis of lupus vulgaris with PKC was made and the patient was started on short course antitubercular therapy (ATT) with rifampicin (10 mg/kg/day), isoniazid (5 mg/kg/day), ethambutol (15 mg/kg/day) and pyrazinamide (25 mg/kg/day) for the initial 2 months, to be followed by rifampicin and isoniazid for 4 months. For eye lesions, topical drops (dexamethasone 0.01% and chloramphenicol 0.5%) twice daily, were prescribed. Follow up after 3 weeks showed complete resolution of eye lesions with residual nebulomacular corneal opacities. The skin lesion resolved after 2 months. Case 2 Hematological investigations and stool examination were unremarkable. Bacterial culture from lid margin and conjunctiva was sterile. X-ray chest revealed multiple opacities in the left upper zone, suggestive of pulmonary tuberculosis. Mantoux test was 22 x 25 mm, with marked induration and vesiculation. FNAC from right inguinal lymph node showed granulomatous infiltrate. Skin biopsies from the ulcer and follicular lesion on trunk revealed caseation necrosis, abscess formation in the center with epithelioid cell granuloma at the periphery and perifollicular tubercular granuloma respectively, corroborating the diagnosis of scrofuloderma with LS. Tissue culture on LJ medium was sterile; however Mycobacterium tuberculosis grew on BACTEC® 460 TB System after one week. Patient was put on short course ATT for 6 months. For PKC, topical steroid and antibiotic drops were prescribed. After 3 weeks of treatment, there was complete resolution of phlyctens, with persistence of residual nebular corneal opacities. The groin ulcer resolved after 3 months, with puckered scarring. Discussion Phlyctenular keratoconjunctivitis is a nonspecific allergic response in the cornea and/or conjunctiva, to a variety of antigens. Conjunctival phlyctens are usually transient and asymptomatic, but occasionally in larger phlyctens, frank pustular conjunctivitis may develop with subsequent penetration into sclera, leading to permanent scar formation. Corneal phlyctens present with lacrimation, photophobia and blepharospasm and tend to leave opacities, leading to permanent vision impairment or occasionally blindness.[7] Tuberculosis as an etiological association, is being supplanted by staphylococcal infection and worm infestation in the developed world. Tuberculosis has been implicated in 77% (86/112) of all cases of PKC from India.[3] PKC lesions were observed to be more severe and recurrent in patients with tuberculosis. The most common underlying tubercular focus was found to be the lungs (56/86), followed by tubercular lymphadenopathy, but none had cutaneous disease.[3] A tuberculid is a cutaneous cell mediated immunological response to a tubercular focus, often occult, elsewhere in the body. Lichen scrofulosorum is the commonest presentation.[2] Thus, both PKC and LS represent delayed hypersensitive immunological response to Mycobacterium tuberculosis in eyes and skin, respectively. This was observed in case 2, in the present report. PKC was considered to be a usual allergic phenomenon, attributed to primary tuberculosis in children over 50 years ago.[4] However, since then, only isolated cases along with papulonecrotic tuberculides have been reported.[5],[6] Of our two cases, one had LS with scrofuloderma, while second had lupus vulgaris alone. Though PKC is most frequently reported in children, most series on pediatric tuberculosis fail to document this entity.[8],[9] The incidence of underlying systemic involvement with cutaneous tuberculosis has varied from 1.7 to 26.1%, with frequent involvement of lungs and lymph nodes.[8],[9],[10] Although most dermatologists diligently look for systemic disease, a detailed ophthalmologic evaluation is often overlooked. We suggest that a simple practice of ophthalmological evaluation in all patients with cutaneous tuberculosis, will result in timely institution of local treatment of PKC and will subsequently ameliorate the unwanted complications of visual disability. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06098f1.jpg] [dv06098f2.jpg] |
| |||||||||

{kind=link}
{kind=link}