 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
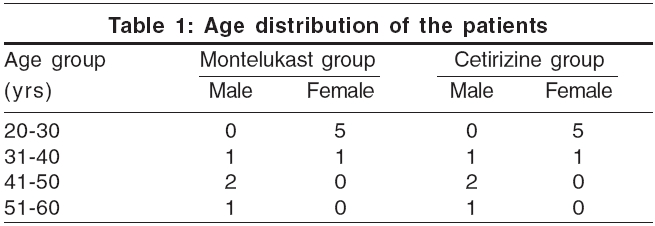
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 4, July-August, 2006, pp. 312-314 Letter To Editor Oral montelukast monotherapy is ineffective in chronic idiopathic urticaria: A comparison with oral cetirizine Godse KiranV Shree Skin Centre, 21 and 22, L Market, Sector 8 Nerul, Navi Mumbai - 400 706 Code Number: dv06107 Sir, Chronic idiopathic urticaria (CIU) is a common cutaneous disorder, for which there is usually no identifiable cause.[1] H 1 -receptor antagonists are recommended as the first-line treatment in CIU. Chronic urticaria, which cannot be classified in any of the known causes, is described as chronic idiopathic urticaria. Recently, antileukotriene receptors such as montelukast, have been used, either as monotherapy, or in combination with H 1 -receptor antagonists. We conducted a study to compare the efficacy of oral montelukast with oral cetirizine in the treatment of chronic idiopathic urticaria. Twenty patients (12 females and 8 males) in the age group of 20 to 60 years (mean age 31.2 years) with chronic urticaria, were enrolled in the study after an informed written consent. Exclusion criteria were physical urticaria, urticarial vasculitis, pregnant or lactating women, a history of sensitivity to aspirin or NSAIDs, a history of aggravation of symptoms by pressure, and a positive cutaneous test to autologous serum. Routine investigations like complete blood count, and urine and stool examination were done to rule out infections. The patients were randomly allocated into two age- and sex-matched groups of 10 patients each [Table - 1]. Randomization was achieved with the help of randomization software. One group was given montelukast 10 mg and the other, cetirizine 10 mg daily in the evening for two weeks. Patients were evaluated at baseline, after a week. and at the end of two weeks. Improvement was monitored by using the urticaria activity score (UAS) which was estimated at weekly intervals. The UAS consisted of the sum of the wheal number score and the itch severity score. The wheal numbers were graded from 0 to 3 as follows: 0, less than 10 small wheals (diameter, < 3 cm); 1, 10 to 50 small wheals. or less than 10 large wheals (diameter,> 3 cm); 2, greater than 50 small wheals or 10 to 50 large wheals; and 3, almost the whole body is covered. The severity of the itching was also graded daily from 0 to 3 (0, none; 1, mild; 2, moderate; and 3, severe). Thus, the UAS ranged from 0 to 6 per week for each patient. Baseline average UAS was 4.6 in the montelukast group and 4.5 in the cetirizine group. Eight out of ten patients in the montelukast group, reported within seven days of starting treatment due to worsening of itching and lesions, with UAS average score going up to 5.5 in eight patients, while two patients did not follow up. These eight patients were started on cetirizine, 10 mg daily in the evening, for control of urticaria. Treatment with montelukast as monotherapy failed to control the urticarial symptoms such as pruritus and hives. All patients in the cetirizine group showed control of symptoms, with UAS average score coming down to average of 2.2. The effects of leukotriene receptor antagonists (LT-RA) in patients with CIU have been evaluated mostly, in a heterogeneous population of patients. The majority are anecdotal reports of chronic urticaria cases, and only a few placebo-controlled studies are reported.[2],[3],[4],[5],[6] Of these studies, four demonstrated a beneficial effect of LT-RAs,[2],[4],[5],[6] whereas one demonstrated that LT-RAs did not benefit the patients.[5] A clinical trial from Italy found that a combination of desloratadine and montelukast does not seem to offer a substantial advantage to desloratadine monotherapy in patients affected by moderate CIU.[7] In this trial, Di Lorenzo and coworkers reported the results of a placebo-controlled, double-blind examination of desloratadine, montelukast, both, or neither in 160 patients with moderate CIU. Desloratadine was clearly the most effective treatment. All of the 80 subjects who received desloratadine, completed the study. There was no additional benefit for any outcome, with the addition of montelukast to desloratadine. Monotherapy with montelukast was more effective than placebo, but montelukast was consistently less effective than desloratadine. Furthermore, 27 of the 40 subjects on montelukast monotherapy failed to complete the 6-week study, as did 35 of the 40 subjects receiving placebo. The results of this study do not support the use of LTRAs as either monotherapy or add-on therapy in moderate CIU, in patients with negative autologous serum skin tests, whose urticaria is not worse when challenged with aspirin or NSAIDs.[7] Moreover, montelukast has been reported to cause urticaria in a case report.[8] This study could not be completed as the montelukast group of patients showed no control of symptoms, and patients demanded the rescue medication i.e., cetirizine. There are no published studies from India about use of montelukast in urticaria. While monotherapy with montelukast is probably not advisable, it needs to be validated in the Indian population, whether addition of montelukast to an antihistamine offers any additional advantage. Larger and better-designed studies are required to settle this question. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06107t1.jpg] |
| |||||||||

{kind=link}