 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 6, November-December, 2006, pp. 410-414 Review Article Immune reconstitution inflammatory syndrome Surjushe AU, Jindal SR, Kamath RR, Saple DG Department of Dermatology, Venereology and Leprosy, Grant Medical College and Sir J J Group of Hospitals, Mumbai, Maharashtra Code Number: dv06145 Introduction Antiretroviral therapy (ART) strengthens the immune system and restores protective pathogen-specific immune responses. This results in decreased incidence of opportunistic infections (OI), decrease in the viral load and increase in the CD4 counts. With restoration of immunity, the body begins to fight aggressively against coexisting infection thereby causing atypical manifestations of opportunistic infections, which may cause severe inflammation in tissue. The constellation of clinical symptoms, signs or investigational parameters resulting from such inflammatory response has been variously called immune reconstitution inflammatory syndrome (IRIS) or immune restoration disease (IRD) or immune rebound illness.[1] IRIS is defined as occurrence or worsening of clinical and/or laboratory parameters despite a favorable outcome in human immunodeficiency virus (HIV) surrogate markers (CD4 counts) and plasma viral load.[2] Both infective (clinical or subclinical) and noninfective conditions can act as triggering factors for precipitating IRIS. History of IRIS After the introduction of highly active antiretroviral therapy (HAART) in the mid-1990s, there were a lot of case reports and case-series dealing with IRIS[3],[4] and the name IRD was given for the phenomenon prior to 2000.[5] Joseph A. De Simone and colleagues from Thomas Jefferson University in Philadelphia were one of the first groups who attempted to define immune reconstitution syndrome in 2000.[6] They found that many HIV-positive people developed a spectrum of illnesses once they responded to HAART. They developed conditions such as Mycobacterium avium complex (MAC) infection and cryptococcal meningitis, at a time when their immune function was actually improving. Initially it was considered to be a Jarisch-Herxheimer or lepra-like reaction. Later it was found to be due to the restoration of immunity thereby eliciting hypersensitivity reaction to an existing microbe or antigen in the body. De Simone and his colleagues named this relatively uncommon phenomenon as immune reconstitution syndrome.[6]Risk factors for IRIS IRIS occurs more frequently in some patients or in some situations. These include: a CD4 count below 50 cells/cmm prior to initiation of HAART,[7] a high viral load before initiation of therapy,[8] undetected presence of antigens of nonviable microorganisms (e.g., cryptococci and CMV), active or subclinical infection by opportunistic pathogens, initiation of ART in close proximity to the diagnosis and initiation of treatment for an OI,[9] use of cytokines such as IL-2 to treat HIV infection and genetic mutations of innate cytokines.Criteria for Diagnosis Recently, French et al have laid down criteria so as to aid the diagnosis.[2] These are: Major criteria
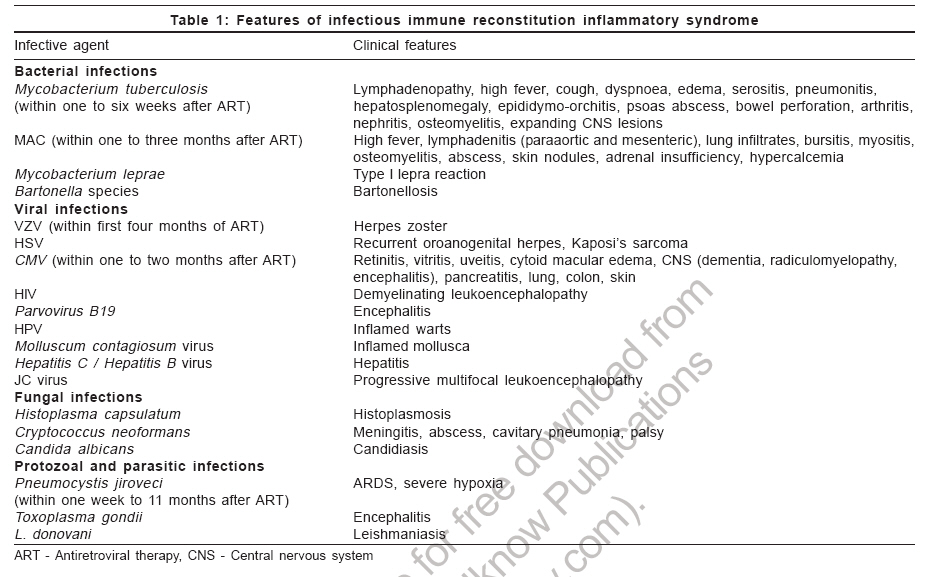
Mechanism of IRIS Although the exact mechanism of IRIS is not known, it may be due to immunologic consequences of HAART such as increase in CD4 cell levels, along with an elevated CD8 cell count and an increased activity of cytokines like IL-2 and interferon-gamma. De Simone and his colleagues noted that a decrease in HIV viral load might alter levels of interleukin 12 (IL-12), a mediator of anti-cryptococcal activity, resulting in meningitis symptoms. Guillaume Foulon and colleagues found that interleukin 2 (IL-2) and interferon-gamma appeared to be the important factors in two patients developing sarcoidosis as IRIS, as both cytokines are essential in the production of a granulomatous response.[10] Presentations of IRIS The clinical features of IRIS differ according to the inflammatory or infective pathology that is responsible for causing it [Table - 1]. Briefly the various presentations include, Noninfectious syndromes: (i) With cutaneous involvement : Papular urticaria, eosinophilic folliculitis, Sweet′s syndrome, Reiter′s syndrome, sarcoidosis, systemic lupus erythematosus, Peyronie′s disease (ii) Without cutaneous involvement : Autoimmune thyroiditis, Guillain-Barrι syndrome, myopathy, radiculopathy, acute porphyria, Non-Hodgkin′s lymphomas, Castleman′s disease Infectious syndromes Various infectious syndromes described in association with IRIS are mentioned in [Table - 1]. Clinical Features of some common IRIS The clinical manifestations of IRIS associated with some common OIs are elaborated below. Tuberculosis and atypical mycobacterial infections[11],[12] Tuberculosis (TB) as IRIS typically occurs one to six weeks after the patient begins ART. The signs and symptoms of tuberculous IRIS may include high fever, new or worsening lymphadenopathy (mediastinal or peripheral), worsening of pulmonary symptoms and infiltrates or new or increasing pleural effusion. Lymph node abscesses usually occur during the first weeks on HAART. Extrapulmonary presentations may occur, including expanding central nervous system lesions, skin or visceral abscesses, osteomyelitis, nephritis, meningitis, hypercalcemia, hepatosplenomegaly, epididymo-orchitis, psoas abscess and bowel perforation. In one study, four out of five patients, who had clinically developed atypical mycobacterial infections after HAART and significant improvements in CD4 T cell levels, showed a significantly increased MAC-specific T cell response in vitro , proving that this phenomenon is indeed caused by the unmasking of subclinical infections. Cryptococcal meningitis[13] Cryptococcal IRIS is usually seen within one week to 11 months after ART. In patients with or without previously diagnosed cryptococcal meningitis, presentation of cryptococcal IRIS typically includes fever, headache, lymphadenitis and meningitis. In cases of IRIS, the MRI usually shows choriomeningitis with significant enhancement in the choroid plexus. Cryptococcal antigen in the cerebrospinal fluid is positive, although culture remains negative. Pneumocystis jiroveci pneumonia[14] Immune reconstitution inflammatory syndrome may present as worsening pulmonary symptoms and high fever in patients who had been improving on PCP therapy or in patients with recent successful treatment of PCP. Chest X-ray may show worsening lung involvement and oxygen saturation or arterial blood gas measurements may show worsening hypoxia or alveolar-arterial oxygen gradient. PCP IRIS, in certain cases, may lead to fatal acute respiratory failure. CMV[15] CMV retinitis may be seen either in patients with a prior history of CMV retinitis or in patients with no previous evidence of retinitis while CMV vitritis and uveitis are seen exclusively in people with previous CMV retinitis infection who responded to ARV therapy. CMV vitritis typically will present with acute onset of blurred vision and "floaters" caused by posterior segment inflammation. Ophthalmologic examination reveals numerous inflammatory cells in the vitreous humor. Symptoms usually resolve in one month without specific treatment and without any lasting visual effects. CMV uveitis as IRIS may occur within months of ART initiation, but typically is a late complication; occurring about three years after patients begin ART. It often results in macular edema, epiretinal membrane formation and/or cataracts, which can lead to permanent vision loss and hence requires a high index of suspicion. Differential diagnosis Failure of ART or toxicity, active opportunistic infection and failure of antimicrobial therapy are considered in the differential diagnosis. Failure of ART can be ruled out with decrease in CD4 count, increase in viral load, along with clinical deterioration while active opportunistic infections can be ruled out by isolating the pathogens. The World Health Organization (WHO) made an important distinction between IRIS and clinical failure while on anti-HIV therapy.[16] "Clinical failure is defined as clinical disease progression with development of an opportunistic infection or malignancy when the drugs have been given sufficient time to induce a protective degree of immune restoration. This needs to be differentiated from an immune reconstitution syndrome which can be seen within the first several weeks after the institution of therapy if a subclinical infection is present at baseline."[16] Treatment of IRIS As of now, there are no standard guidelines for the treatment of IRIS and the following interventions are mostly based on published case reports and other anecdotal clinical evidence. Treatment includes continuation of primary therapy against the offending pathogen in order to decrease the antigenic load, continuation of effective HAART and judicious use of anti-inflammatory agents.[17]
Prevention of IRIS Diagnosis of IRIS requires a high index of suspicion. Detailed clinical history should be taken in patients suspected to have IRIS, which includes the following: Symptoms: fever, cough or any specific symptoms; history of OIs: including recently diagnosed as well as past OIs; treatment of OIs: date of initiation, duration of therapy, clinical response, adherence, defaulter, resistance; ART initiation: date, regimen, adherence, prior history of ART, toxicity, any drug interaction; CD4 count and HIV viral load prior to ART initiation. Look for the vital signs, including temperature, heart rate, blood pressure and respiratory rate. Perform a careful and thorough physical examination based on symptoms and suspicion of systems involved. Ophthalmologic examination should be included in all patients. The following investigations should be considered before starting ART: Complete blood count with differential, ESR, serum electrolytes, liver function tests and renal function tests, CD4 count and HIV viral load, chest X-ray, Mantoux (tuberculin) test, sputum stain and culture and ultrasonography of abdomen. In a suspected case, even an initially negative Mantoux test becoming positive could be suggestive of IRIS. Patients who are started on ART having CD4 count of less than 100 cells/µl require close clinical monitoring during the first weeks of ART. Similarly, they should be counseled about the risk of development of IRIS to avoid being discouraged and defaulting on therapy as development of IRIS suggests increase in the immunity and is a good sign unless life-threatening. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06145t1.jpg] |
| |||||||||

{kind=link}