 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
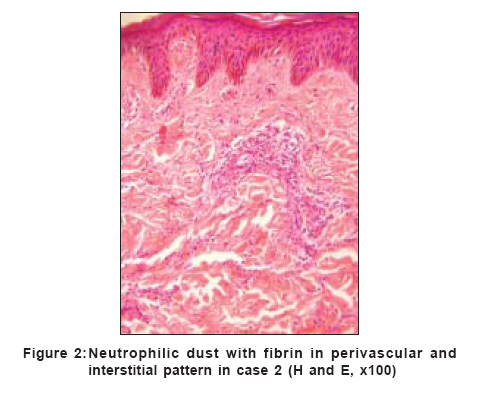
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 6, November-December, 2006, pp. 437-439 Case Report Cutaneous vasculitis as a presenting feature of multiple myeloma: A report of 2 cases Kembre PriyamS, Mahajan Sunanda, Kharkar Vidya, Khopkar Uday Department of Dermatology, Venereology and Leprology, GS Medical College and KEM Hospital, Parel, Mumbai Code Number: dv06150 Abstract We report two male patients who presented with symmetrical, painful purpura that evolved into bullae and necrotic ulcers, predominantly on the extremities, over two months in spite of conventional therapy including oral steroids. Examination showed livedoid and purpuric patches with necrotic centers in starburst pattern over the extremities and buttocks. The first case also had similar lesions over the ears. The clinical presentation and the histopathological examination suggested a diagnosis of necrotizing leukocytoclastic vasculitis (LCV). Blood testing ruled out connective tissue disease, hepatitis B or C infection or streptococcal infection as underlying cause of vasculitis. Serum antinuclear factor, antineutrophilic cytoplasmic antibody and anticardiolipin anticoagulant were negative in both cases. Cryoglobulins were positive in case 2. An incidental finding was raised serum proteins and globulins in case 2. Further investigations revealed M band on electrophoresis and features of multiple myeloma on bone marrow biopsy in both cases. These cases emphasize the importance of simple investigations like serum proteins in the evaluation of LCV.Keywords: Leukocytoclastic vasculitis, Multiple myeloma, Palpable purpura Introduction Patients commonly present to dermatologists with purpura secondary to leukocytoclastic vasculitis (LCV). A thorough workup is needed to diagnose the underlying condition. We report two patients presenting with LCV who were found to have multiple myeloma on investigation. Multiple myeloma rarely presents as LCV.[1] However, the diagnosis must be suspected in a patient who does not respond to conventional therapy.Case reports Case 1 A 52-year-old male presented with multiple painful red raised lesions on the extremities and the ears since two months. The patient had received various therapies at other clinics including antibiotics and oral steroids (prednisolone 40 mg/day) without any response. There was history of weight loss and bloody diarrhea on and off since the last four months. He also complained of low-grade fever, malaise and arthralgias involving the back and knees since one month. Examination revealed edema of both feet and pallor. Palpable purpura was noted over the extremities, [Figure - 1] which eventually progressed to developing necrosis and ulcerations. Investigations revealed anemia (hemoglobin 10. 7 gm%), neutrophilic leukocytosis (WBC count 29,200/ mm 3 P-87, L-10, M-3) and normal platelet count. Serum total proteins, albumin and globulin, blood urea and serum creatinine were normal. Urine routine and 24h urine proteins were normal. Skin biopsy was indicative of leukocytoclastic vasculitis. Rheumatoid factor, hepatitis B surface antigen, anti-HCV antibodies and HIV-ELISA were also negative. Antinuclear antibody, lupus anticoagulant and cryoglobulins were also negative. C-reactive protein was raised. Serum protein electrophoresis revealed M-spike. Urine protein electrophoresis showed Bence Jones protein. Bone marrow study revealed 20% plasma cells. Radiological evaluation was normal. He was diagnosed as Stage I multiple myeloma and started on vincristine, adriamycin and 50 mg of oral prednisolone with low molecular weight heparin and gabapentin. The palpable purpura progressed to develop necrosis of the acral portions of the extremities with ulcerations which healed within three months of treatment. Case 2 A 42-year-old farmer presented with painful ulcerations over the legs since two months and over the arms and forearms since 15 days. Examination revealed large geographic ulcerations over the upper and lower extremities covered with thick hemorrhagic crusts and gangrene of the tips of the digits. He also had punctate ulcerations over the palate and subconjunctival hemorrhages in the left eye. Investigations revealed anemia (hemoglobin 7.2 gm%), neutrophilic leucocytosis (WBC count 17,300; P-80, L-170, M-3) and platelet count of 75,000/cumm. Total proteins were raised to 8.7 gm% with a reversal of albumin: globulin ratio (1:3). Blood urea and serum creatinine were normal. The 24h urine protein was normal. Cryoglobulins were positive. Hepatitis B surface antigen and antibodies to HCV and HIV- ELISA were negative. The antinuclear factor (ANA) and anticardiolipin antibody were also negative. C-reactive protein was raised. Skin biopsy showed neutrophilic infiltrate and nuclear dust around vessel walls indicative of leukocytoclastic vasculitis. [Figure - 2] Indirect immunofluorescence showed cytoplasmic staining for antineutrophil cytoplasmic antibody (ANCA). Serum immunoglobulins were raised with IgG predominance. Serum protein electrophoresis revealed M-spike. Urine protein electrophoresis showed Bence Jones protein. Bone marrow study showed decrease in erythroid precursors with 28% plasma cells. The marrow was hypercellular with abundant immature and mature plasma cells Radiological evaluation was normal. He was diagnosed as multiple myeloma and started on intravenous dexamethasone 8 mg 8-hourly. He developed dyspnea on exertion (Grade 3). X-ray chest showed left-sided pleural effusion. Echocardiogram revealed poor ejection fraction (30%). He continued to develop nonhealing ulcerations. In time, his entire limb showed a black discoloration with necrosis. Ultimately, he succumbed to cardiopulmonary failure secondary to pulmonary edema with left ventricular failure. Discussion Leukocytoclastic vasculitis (LCV) has many associations, including the rarely observed multiple myeloma (MM). The close temporal relationship of cancer and vasculitis in such patients indicates that vasculitis may be a paraneoplastic condition. Failure of a vasculitis to respond to conventional therapy should raise suspicion about underlying malignancy.[1],[2] Amongst others investigations in a case of LCV include those for detecting underlying solid and hematological malignancies. Investigations that lead to the diagnosis of multiple myeloma, include complete blood count to rule out anemia, thrombocytopenia or leucopenia, total protein, albumin and globulin, blood urea, creatinine and uric acid. In our second patient it was the high globulin level that raised the suspicion of myeloma. Kitamura has reported the utility of screening investigations like abnormal flocculation tests and hyperglobulinemia in the detection of multiple myeloma.[3] Serum protein electrophoresis, urine protein electrophoresis and immunofixation determine the type of protein present. Quantitative immunoglobulin (i.e., IgG, IgA, IgM) levels are used for monitoring response to therapy. Beta-2 microglobulin is a surrogate marker for the overall body tumor burden. C-reactive protein is a surrogate marker of interleukin 6 activity and is useful for prognostication. Skeletal survey can be used to detect diffuse osteopenia or discrete osteolytic lesions. Cutaneous manifestations are rare in multiple myeloma and consist of multiple erythematous or violaceous nodules or plaques. LCV is even rarer in multiple myeloma. In a study of 2357 patients with a diagnosis of MM, only eight patients were found to have LCV.[4] Leukocytoclastic vasculitis has been reported twice as the first manifestation of multiple myeloma.[1],[5] Marini et al . reported two female patients who presented with recurrent palpable purpura, ulcers and necroses on the extremities who were later diagnosed to have multiple myeloma.[1] Birchmore et al . reported a case of a man with IgA kappa multiple myeloma presenting with a five-year history of relapsing Henoch-Schonlein purpura and polyarteritis nodosa as early manifestations of the disease. The patient also had multisystem large vessel vasculitis (ANCA negative) producing aneurysms of renal and hepatic arteries.[6] Leukocytoclastic vasculitis is a rare histopathogical finding in cases of multiple myeloma and indicates a poorer prognosis and short survival independent of the therapy.[7] This report highlights the importance of simple investigations such as plasma proteins in the evaluation of LCV and emphasizes the need to investigate patients who do not respond well to conventional therapy. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06150f2.jpg] [dv06150f1.jpg] |
| |||||||||

{kind=link}
{kind=link}