 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
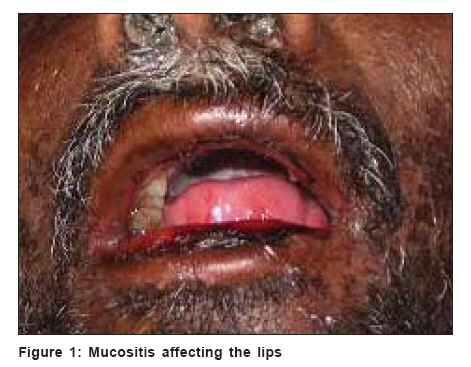
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 6, November-December, 2006, pp. 440-442 Case Report Bullous variant of acral erythema due to methotrexate Kuruvila Sheela, Dalal Monica, Sivanesan B Department of Dermatology, Pondicherry Institute of Medical Sciences, Pondicherry Code Number: dv06151 Abstract Chemotherapy-induced acral erythema is a painful erythema of the palms and soles which occurs following chemotherapy. It is usually seen due to cytarabine, doxorubicin and fluorouracil. We present a 40-year-old male patient, a biopsy proven case of squamous cell carcinoma of the floor of the mouth, who developed a bullous variant of acral erythema after a single intravenous dose of methotrexate. He also had fever, buccal mucositis, leucopenia, thrombocytopenia and hyperpigmented macular rash on the face and upper trunk. The bullous variant of acral erythema due to methotrexate has rarely been reported.Keywords: Acral erythema, Methotrexate Introduction Methotrexate-induced acral erythema (AE) is an uncommon manifestation of a commonly used drug in medical practice. Other chemotherapeutic agents such as cytarabine, doxorubicin and fluorouracil have been implicated more frequently.[1],[2],[3] The bullous variant is even more uncommon, with sporadic cases having been reported in the literature. The present case is the first report from India.Case report A 40-year-old male patient, a biopsy proven case of squamous cell carcinoma of the floor of the mouth, was advised therapy with intravenous methotrexate followed by radiation therapy. He was treated with a single dose of 100mg of intravenous methotrexate. No other chemotherapeutic agents were administered. The patient developed fever within 24h of receiving the injection and burning pain over both soles three days later. On examination, the patient was found to have severe mucositis involving the lips and oral mucosa [Figure - 1]. There were symmetrical, well-defined erythematous tender macules on the tips of the toes and both soles [Figure - 2]. A few of these macules had central bullae. There was a single erythematous macule on the right palm. There was also a hyperpigmented nonpurpuric macular rash on the face and upper trunk [Figure - 3]. Investigations revealed a total leukocyte count of 900/cu mm and a platelet count of 1.3 lakhs/cu mm which subsequently dropped to 400/cu mm and 15,000 platelets/cu mm respectively over a period of five days. All other investigations including liver function tests were normal. Histopathological examination of the skin lesions could not be done in view of the low platelet count. The patient recovered within two weeks with supportive therapy for the associated leucopenia and thrombocytopenia. Discussion Chemotherapy-induced AE was first described in 1982.[1],[2] This is a distinctive toxic reaction which manifests as a painful AE.[1] It is most commonly seen with high-dose cytarabine, doxorubicin and fluorouracil.[1],[2],[3] The exact mechanism of this reaction is unknown but concentration of the drug by the large number of sweat glands in the palms and soles may explain the localization of the reaction.[1],[2],[4] This hypothesis is supported by the association of AE with chemotherapy-induced syringosquamous metaplasia.[1] This reaction is dose-dependent and may appear with bolus high-dose infusions or long-term low-dose infusions.[2],[5] It is reported mostly in adults and appears 1 to 21 days after the administration of the chemotherapy. It presents as painful, edematous, symmetrical, well-demarcated erythematous macules on the palms and soles. This is often preceded by dysaesthesia and tingling over the palms and soles.[1],[2],[5] In severe cases, bullae involving the palms, soles and the dorsal aspect of the hands and feet may develop.[1] The patient usually recovers without complications although full thickness ischemic necrosis may occur rarely in areas of blistering.[5] Most cases require only supportive care like cold compresses and elevation of the affected limb. Mucositis, thrombocytopenia and leucopenia are well-known adverse effects of methotrexate. However, the association of AE with methotrexate therapy is unusual.[2],[6],[7],[8],[9],[10] Acral erythema involving the soles of the feet with sparing of the palms and the concomitant presence of diffuse macular lesions over the body has been reported in one case previously.[2] The bullous variant of AE has been commonly described for regimens containing cytarabine. Four case reports of bullous AE due to methotrexate have been published previously.[2],[6],[9],[10] In our patient there was bullous AE involving the soles of both feet with only a single erythematous macule on the right palm in addition to a macular rash on the face and upper trunk, buccal mucositis, leucopenia and thrombocytopenia. Methotrexate was not reinstituted in this patient and the patient was referred for radiotherapy. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06151f3.jpg] [dv06151f1.jpg] [dv06151f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}