 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
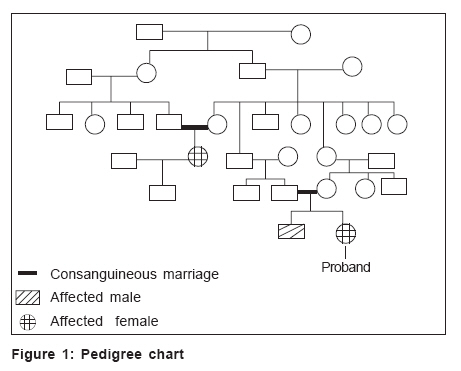
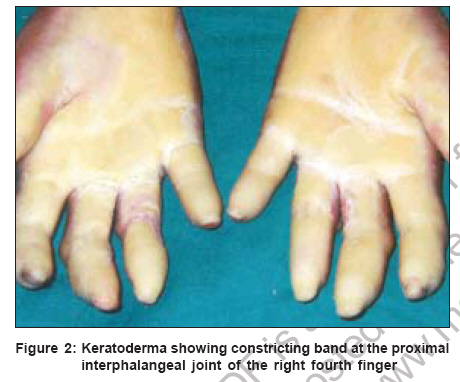
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 6, November-December, 2006, pp. 449-451 Case Report Variant of Vohwinkel's syndrome Ali MirMubashir, Upadya GathaM Department of Dermatology, Kasturba Medical College Hospital, Attavar, Mangalore Code Number: dv06154 Abstract A 28-year-old female born to consanguineous parents, presented with progressive palmoplantar keratoderma since the age of six months and a constricting band on right fourth finger of one year duration. There was history of similar complaints being present in two other family members. Associated clinical findings included starfish-shaped cornified plaques on knuckles, resorption of distal phalanges and keratotic plaques on elbows, groins and knees. The patient was mentally sound and had normal audiometry. Biopsy from hyperkeratotic plaque showed hyperkeratosis, parakeratosis, increased granular layer and papillomatosis. Gene mapping for loricrin mutation was found to be negative.Keywords: Keratoderma, Palmoplantar, Vohwinkel′s syndrome Introduction Keratoderma hereditaria mutilans (KHM) was first described by Vohwinkel in the German literature in 1929.[1] This palmoplantar keratoderma is thought to be an autosomal dominant genodermatosis with defective epidermal differentiation and is quite rare.[2] A triad of clinical features is essentially pathognomonic for Vohwinkel′s syndrome and this includes diffuse "honeycomb-like" thickening of palms and soles, "starfish-shaped" keratotic plaques on the dorsum of hands and feet and fibrous constricting bands (pseudo-ainhum) at the interphalangeal joints of hands and feet.[2],[3] The disease is seen in early childhood and has a familial tendency.[3] Associated findings with the disease are cicatricial alopecia,[4] ichthyosiform dermatoses, high-tone acoustic impairment, deaf mutism, spastic paraplegia and myopathy, knuckle pads and nail anomalies.[5] The hyperkeratosis in patients with KHM is difficult to treat.Case report A 28-year-old female born to consanguineous parents presented with progressive thickening of palms and soles since the age of six months and a constricting band on the proximal interphalangeal joint of the right fourth finger of one year duration. There was no history of deaf mutism, mental retardation, spastic paralysis or myalgias, cicatricial alopecia, ichthyosiform dermatoses or autoamputation of digits. Two of her second-degree relatives had similar problems [Figure - 1]. Physical examination revealed that the volar aspect of the constricting band was opened and cracked [Figure - 2]. Associated with the keratoderma, the patient also had "starfish-shaped" cornified plaques on the knuckles, resorption of distal phalanges and keratotic papules and plaques on the elbows, groin, knees and feet [Figure - 3]. Biopsy of hyperkeratotic papules showed hyperkeratosis, parakeratosis, increased granular layer and papillomatosis. X-ray of both hands showed acral osteolysis. Audiometry revealed hearing in both ears to be within normal limits. To identify an underlying mutation in the loricrin gene in this patient, genomic DNA was isolated from peripheral blood lymphocytes of the proband using PureGene ® DNA isolation kit. The entire loricrin gene was polymerase chain reaction amplified from genomic DNA and sequenced directly in an ABI Prism 310 automated sequencer, using the ABI prism big dye terminator cycle sequencing ready reaction kit, following purification with centriflex gel filtration cartridges. Gene mapping for loricrin mutation was found to be negative. Discussion There are thought to be two different forms of Vohwinkel′s syndrome. The type that is associated with sensorineural hearing loss is thought to result from a mutation of GJB2 gene that codes for the gap junction protein, connexin 26.[6] Cases of connexin 26 mutations causing autosomal dominant palmoplantar keratoderma with deafness but without other clinical features of Vohwinkel′s syndrome have also been reported.[7] The other clinical variant of Vohwinkel′s syndrome associated with generalized ichthyosis without deafness is caused by mutations of the gene encoding loricrin.[8] The differential diagnosis of Vohwinkel′s syndrome includes other types of hereditary keratodermas that may be associated with autoamputation of the digits. These are Olmsted′s syndrome, acral keratoderma of Sybert, Mal de meleda and palmoplantar keratoderma of Gamborg Nielsen.[9] Vohwinkel′s syndrome has variable expression and treatment should focus on palliation of the keratoderma and prevention of autoamputation. Surgical release of the constricting bands may be used to prevent autoamputation. Treatment options for keratoderma include keratolytics and retinoids. Etretinate and isotretinoin have been used successfully in several patients with Vohwinkel′s syndrome to reverse both the keratoderma and pseudoainhum; however, the condition recurred once the medication was discontinued.[2],[3],[10],[11] Acknowledgments We would like to acknowledge Dr. Angela Christiano for the help rendered by her in gene mapping of the loricrin mutation.References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06154f2.jpg] [dv06154f1.jpg] [dv06154f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}