 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
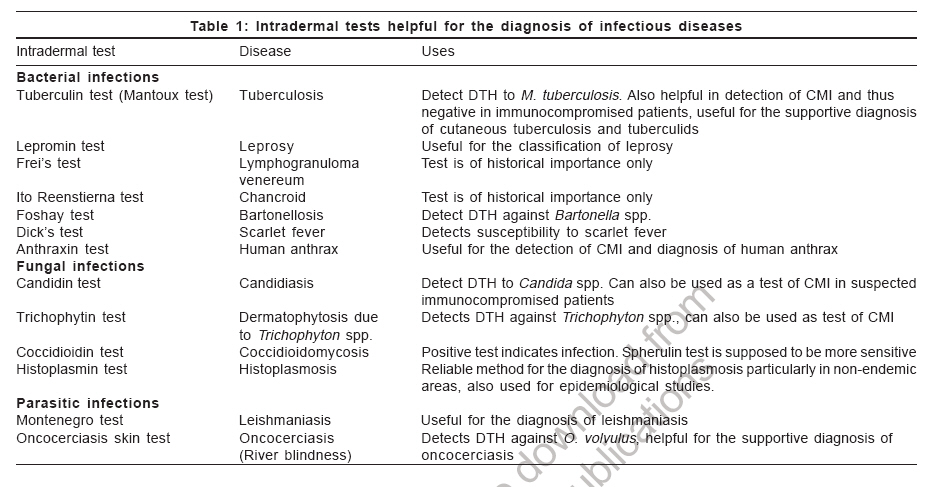
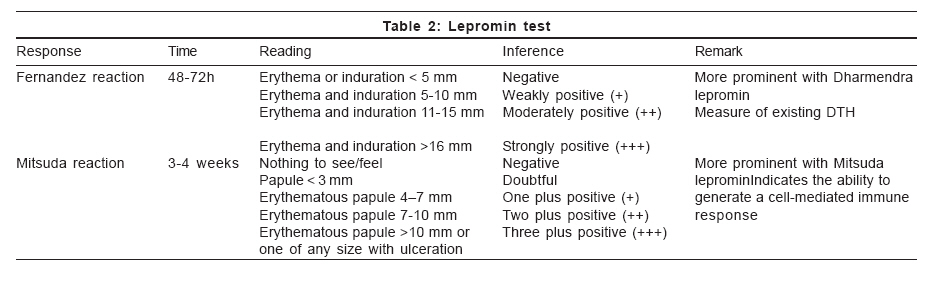
Indian Journal of Dermatology, Venereology and Leprology, Vol. 72, No. 6, November-December, 2006, pp. 461-465 Resident's Page Intradermal tests in dermatology-I: Tests for infectious diseases Nagar Rahul, Pande Sushil, Khopkar Uday Department of Dermatology, Seth GS Medical College and KEM Hospital, Mumbai Code Number: dv06161 Introduction Intradermal tests are widely used to support the diagnosis of dermatological and nondermatological diseases. They are mainly indicated for the detection of immediate (Type I hypersensitivity) and delayed type hypersensitivity (DTH, Type IV hypersensitivity) towards exogenous or endogenous antigens. Intradermal tests for the diagnosis of infectious diseases in relevance to dermatovenereology are discussed in this section. Intradermal tests for the diagnosis of infectious diseases are listed in [Table - 1]. They are indicated to detect DTH to organisms or their antigens. Before undertaking intradermal test, it is advisable to stop or avoid systemic steroids or immunosuppressive agents at least three days before the procedure as moderate to large doses of corticosteroids may inhibit a DTH reaction. Procedure The uniform feature of all intradermal tests is the injection of the antigen into the superficial layer of the dermis through a fine-bore (26 or 27-G) needle with its bevel pointing upwards. The quantity injected may vary from 0.01 to 0.1 ml but conventionally 0.1 ml is universally used. Although the tests could be done at any site, the proximal part of the flexor aspect of the forearm is conventionally used. This site can be conveniently exposed and the skin of the proximal area is more sensitive than the distal. Interpretation of intradermal tests The optimal time for reading the reaction depends upon the pharmacological agent used for the test and the type of immunological reaction to be observed. Intradermal tests for the detection of DTH are read at 48h, although they can be read as early as 12h and as late as four days. (The lepromin test is read at four weeks and depends on the formation of a granuloma, which is a measure of cell-mediated immunity.) The size of the induration is more important than erythema while interpreting Type IV hypersensitivity. Some of the commonly used intradermal tests in dermatovenereology are briefly discussed here. Intradermal tests for bacterial infections Tuberculin test[1],[2],[3],[4],[5] Tuberculin test, also known as Pirquet′s test/reaction or scarification test, was used by von Pirquet in 1907. The antigen used, tuberculin, is a purified protein extract of bacilli grown on 5% glycerol broth. One tuberculin unit is injected intradermally on the flexor aspect of the forearm and a reading taken after 48h (Mantoux method). Induration measuring more than 10 mm in diameter is considered to be a positive response while that measuring less than 5 mm is considered as negative. A positive test indicates past or present infection with M. tuberculosis or vaccination with bacillus Calmette-Guerin (BCG); an induration of more than 15 mm is usually not due to BCG vaccination. A positive test does not indicate active infection except in children younger than two years. Readings between 6 mm and 9 mm are doubtful and could be because of an atypical mycobacterial infection. A tuberculin test represents DTH but this response is irrelevant to the protective immunity against M. tuberculosis. A negative tuberculin test indicates non-exposure or decreased or absent delayed hypersensitivity to M. tuberculosis as in HIV infection/AIDS, disseminated tuberculosis, primary immunodeficiency disorders of CMI, lymphoreticular malignancies, sarcoidosis, etc. A negative tuberculin test can also occur due to technical errors. A repeat test is not advocated before one week as the tuberculin injected for the first test has a booster effect on the subsequent dose. Tuberculins from atypical mycobacteria or environmental bacteria have also been prepared. They include PPD-B for Battey mycobacteria, PPD-Y for M. kansasii , scrofulin for M scrofulaceum and burulin for M. ulcerans . It is a prognostic test that is very helpful in classifying leprosy. It cannot be used for diagnostic purpose since it is positive in a significant number of normal people and is negative towards the lepromatous pole of the disease. Two types of antigens are available: Mitsuda lepromin, an autoclaved suspension of tissue (whole bacilli) obtained from experimentally infected armadillos (Lepromin A); and Dharmendra lepromin, a purified chloroform-ether extracted suspension of M. leprae (fractionated bacilli with soluble protein component). The response after intradermal injection is typically biphasic, with an early Fernandez and a late Mitsuda reaction [Table - 2]. Both responses are manifestations of CMI towards the antigen. In India, lepromin antigen is prepared by the Central Leprosy Teaching and Research Institute, Chengalpattu, Tamil Nadu. Frei′s test[8] Frei′s test was developed in 1925 for lymphogranuloma venereum (LGV) and uses Frei′s antigen. It indicates delayed hypersensitivity to an intradermal standardized antigen prepared from chlamydia grown in the yolk sac of a chick embryo. The test is read after 48h and again on the fourth day. A nodule more than 5mm at fourth day is considered a positive response. A positive test indicates past or present chlamydial infection. Frei′s test becomes positive two to eight weeks after infection. Frei′s antigen is common to all chlamydial species and is not specific to LGV. Due to its nonspecific nature, the test is no longer used. Ito Reenstierna test Also known as Ducrey′s test, this test was developed to detect hypersensitivity against Haemophilus ducreyi, the causative organism of chancroid. A response indicates cell-mediated hypersensitivity against H. ducreyi and is due to past or current infection with the organism. The antigen is not commercially available. The anthraxin skin test, which measures DTH to anthrax antigens, has been used as a diagnostic tool. It has also been recommended by the WHO for evaluation of immunological memory against anthrax. Anthraxin, a cell wall extract from the vegetative, noncapsulated strain of B. anthracis (Sterne strain), consists mainly of a complex of peptidoglycans and polysaccharides. Anthraxin is prepared by using a cell wall extract in place of the vaccine antigen. Therefore, the anthraxin skin test can differentiate between exposed and unexposed individuals, even if they have been immunized. The anthraxin skin test becomes positive in most of the cases (80%) in the first three days of the disease, and stays positive for a long time after recovery from the disease. Thus, the anthraxin skin test appears to be a valuable method for early diagnosis of acute anthrax and is the only method for the retrospective diagnosis of human anthrax. Foshay test[11] The test involves intradermal injection of a suspension of killed Bartonella henselae , the causative agent of cat-scratch disease. The antigen is prepared from the sterile lymph node material obtained from a patient of cat-scratch disease. The appearance of an area of erythema more than 5 mm diameter after 48h at the injection site is considered a positive reaction. A positive test is a sign of past or present infection. The test is of historical importance only, as it is no longer used for diagnosis because of concerns about the transmission of the organism. Dick′s test This test was devised in 1924 to identify children susceptible to scarlet fever, but is of historical value as scarlet fever is no longer a common or serious disease. The antigen used is pyrogenic exotoxin or Dick′s or scarlatinal toxin of Streptococcus pyogenes . It is also known as erythrogenic toxin because intradermal injection causes an erythematous reaction in a susceptible person. About 0.1 cc of the toxin in the dilution of 1:1000 is injected intradermally on the forearm and the response is read after 24h. The reaction is considered positive when there is an erythema more than 5 mm in diameter and strongly positive if induration also develops. A positive reaction develops after 8-12h and reaches its maximum after 24h. It is negative in convalescent patients and in insusceptible individuals. Intradermal tests for fungal infections This test is performed to detect allergic hypersensitivity towards dermatophytes. Trichophytin antigen is a glycopeptide extracted (using acetone-ethylene glycol extraction method) from the spores and mycelia of dermatophytes, mostly Trichophyton mentagrophytes. Trichophytin in the concentration of either 10 µg, 1 µg or 0.1 µg in 0.1 ml of normal saline is injected intradermally into the flexor forearm. The test is read after 20 min for an immediate reaction and after 24 or 72h for a delayed response. Erythema, edema or induration may be seen and a papulovesicular or ulcerative lesion can also occur. A wheal larger than 10 mm in diameter at 20 min and induration more than 5 mm at 72h is considered a positive response. Hypersensitivity towards Candida albicans is universal. Hence, a test cannot be used to diagnose the infection. The candidin test serves as an aid to evaluate the cellular immune response in patients suspected of having reduced CMI. Candidin is used as a recall antigen for detecting DTH by intradermal testing. Candidin is made from the culture filtrate and cells of two strains of Candida albicans . Compared with healthy controls, reactivity to candidin is significantly reduced in patients with AIDS, and patients with Hodgkin′s disease or sarcoidosis (tuberculin sensitivity is more reliable in the latter case). The test dose of 0.1 mL (Candin ® Allermed Laboratories, Inc., San Diego, California) is injected intradermally on the forearm intended to elicit an induration response in excess of 5 mm at 48h after injection in immunocompetent persons with cellular hypersensitivity to the antigen. There are two antigens available: coccidioidin and spherulin. Coccidioidin is prepared from autolysates of the mycelial phase (saprophytic phase) of Coccidioides immitis , and spherulin, a more sensitive reagent, from the spherule phase (parasitic phase). A positive test is helpful in detecting exposure to the fungus Coccidioides immitis . It can help in differentiating the chronic pulmonary disease caused by this fungus from other chronic cavitary, nodular and fibrotic diseases like tuberculosis and malignancies. The test is negative in patients with disseminated disease or in patients with thin-walled cavities. Histoplasmin test[19],[20],[21] Histoplasmin skin testing is useful in epidemiological studies, such as investigations of case cluster or the definition of endemic areas but is not predictive of histoplasmosis. An antigen containing the M and H precipitins of Histoplasma capsulatum tends to elicit both immediate and delayed hypersensitivity, and hence more false-positive reactions. An antigen that is deficient in the M component can reduce this problem. Intradermal tests for parasitic infections Leishmanin test (Montenegro test)[22],[23],[24] The first study of this test in humans was carried out by Montenegro in 1926 in Brazil. Leishmanin, which is provided by the Pasteur Institute of Teheran, Iran, contains killed Leishmania. A positive reaction consists of a palpable nodule more than 5 mm in diameter developing in 48 to 72h and indicates DTH, but not necessarily immunity, to leishmania organisms. The test is not species-specific. It becomes positive early in the course of cutaneous or mucocutaneous leishmaniasis (except in diffuse cutaneous leishmaniasis) and only after recovery from visceral leishmaniasis. It is highly sensitive for cutaneous leishmaniasis. It is a useful and important tool for epidemiological, immunological, and diagnostic studies and is an essential component of vaccine trials. However, it cannot distinguish between present and past infection. The intradermal test with products from Onchocerca volvulus is highly sensitive in the detection of active onchocerciasis. However, a few reports indicate decreased CMI to parasite-derived antigens, delayed skin-test reactivity, and response to unrelated antigens during Onchocerca volvulus infection. Intradermal tests in various skin or systemic infections thus serve an important role in reaching a diagnosis and predicting the prognosis of these conditions. References
Copyright 2006 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv06161t1.jpg] [dv06161t2.jpg] |
| |||||||||

{kind=link}
{kind=link}