 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
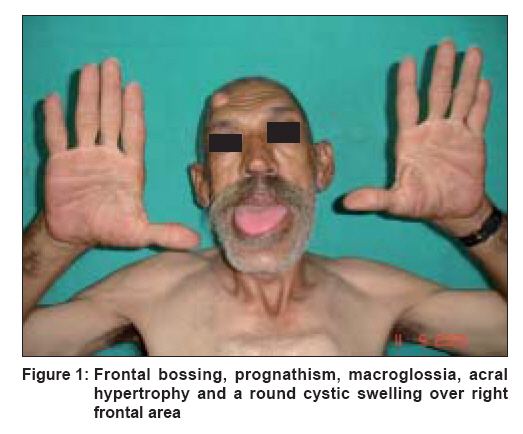
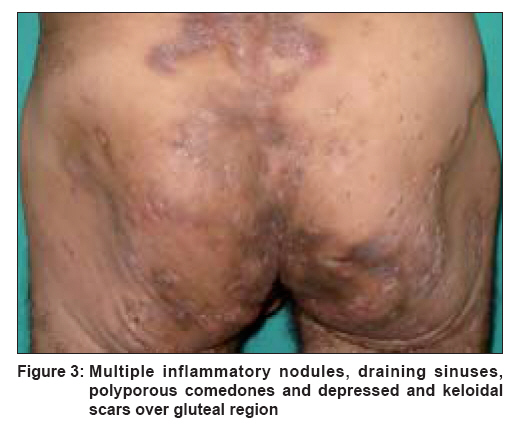
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 139-141 Case Report Late onset isotretinoin resistant acne conglobata in a patient with acromegaly Jain Kapil, Jain VK, Aggarwal Kamal, Bansal Anu Department of Dermatology, Venereology and Leprology, Pt. B.D.S. Post Graduate Institute of Medical Sciences, Rohtak, Haryana Code Number: dv08050 Abstract A 55 year-old male presented with multiple pus-discharging abscesses and sinuses and mutilating scarring on the gluteal region and back prevalent for the last ten years with exacerbations and remissions. Physical examination revealed acromegaly with frontal bossing, prognathism, a barrel chest and acral hypertrophy. Dermatological examination revealed cutis verticis gyrata, thick eyelids, a large triangular nose, a thickened lower lip, macroglossia, widely spaced teeth and widened skin pores with wet and oily skin. Hair was fine and nails were flat and wide. There were multiple inflammatory papules, tender nodules, draining sinuses, and grouped, polyporous comedones as well as multiple and extensive depressed and keloidal scars localized predominantly over the gluteal region with a few scattered lesions over the back. A computed tomography (CT) scan showed widened sella turcica. His basal fasting growth hormone (GH) levels were markedly raised (230 ng/mL; normal 1-5 ng/mL) while the prolactin levels were moderately raised (87 ng/mL; normal 2-5 ng/mL). These findings were consistent with a diagnosis of acromegaly. The patient was put on antibiotics, nonsteroidal antiinflammatory drugs and isotretinoin at a dose of 1 mg/kg/day, which was increased to 1.5 mg/kg/day. Except for an initial mildly beneficial response, the skin lesions were largely resistant to high doses of isotretinoin at the end of four months. Keywords: Acne conglobata, Acromegaly, Cutis verticis gyrata Introduction Acne conglobata (AC) is a rare and severe form of acne seen predominantly as familial cases in males with only a few cases being reported in females. It is a highly inflammatory disease with nodules, abscesses, draining sinus tracts and comedones; healing results in severe scarring. AC is frequently associated with hidradenitis suppurativa and dissecting cellulitis of scalp completing the follicular occlusion triad. [1] Pyoderma gangrenosum (PG) has been reported with AC. [2] Recently, a new entity - the PAPA syndrome has been described, linking pyogenic arthritis, PG and AC. [3] Acne conglobata, especially during exacerbation, may be associated with arthralgia or arthritis, which resembles seronegative spondyloarthropathies. [4] Herein, we report an unusual presentation of acne conglobata associated with acromegaly.Case Report A 55 year-old male presented with multiple pus-discharging abscesses and sinuses and mutilating scarring on the gluteal region and back prevalent for the past ten years with multiple exacerbations and remissions. The patient complained of low back pain and joint pains predominantly involving the hip joints during periods of exacerbation. There was no antecedent history of acne vulgaris and no family history of similar lesions. The patient had no other systemic manifestations including fever, diarrhea and uveitis. Physical examination revealed acromegaly with frontal bossing, prognathism, a barrel chest and acral hypertrophy [Figure - 1]. A round cystic swelling, 25 mm in diameter, was present on the right frontal area. Dermatological examination revealed cutis verticis gyrata [Figure - 2], thick eyelids, a large triangular nose, a thickened lower lip, macroglossia, widely spaced teeth as well as widened skin pores with wet and oily skin. Hair was fine and nails were flat and wide. Furthermore, there were multiple inflammatory papules, tender nodules, draining sinuses; and grouped, multiple, fused black heads and extensive depressed and keloidal scars localized predominantly over the gluteal region with a few scattered lesions over the back [Figure - 3]. The discharge was foul-smelling and sero-purulent. Axillae and groins were spared. A clinical diagnosis of acromegaly with acne conglobata was made. Laboratory analysis revealed leukocytosis (14,000/mm³) with neutrophilia and lymphopenia, moderate anemia (Hemoglobin: 10 g/dL), an elevated ESR (35 mm at the end of one hour) and an elevated C-reactive protein. The patient was found to be diabetic with raised fasting (226 mg/dL) and postprandial (340 mg/dL) blood sugar levels. Urine analysis was normal. Biochemical screening showed no abnormality. Rheumatoid and antinuclear factors as well as HLA-B27 antigen were absent. Bacteriological culture from a pustule showed coagulase-negative staphylococci. Histopathological examination of a typical skin lesion revealed ducts and cystic lesions in the middle and lower dermis lined by keratinizing epithelium and an inflammatory infiltrate mainly consisting of neutrophils, consistent with the diagnosis of acne conglobata. The patient was hypertensive. Heal pad thickness was increased (28 mm; normal for males < 23 mm). A CT scan of the head revealed widened sella turcica. Radiological examination of the affected joints and spine was normal and no periosteal thickening was visible on the X-ray of the feet. Serum IGF-1 level was mildly raised (575 ng/mL; normal 71-290 ng/mL) while basal fasting growth hormone (GH) levels were markedly raised (230 ng/mL; normal 1-5 ng/mL). Prolactin levels were moderately raised (87 ng/mL; normal 2-5 ng/mL) and these findings were consistent with the diagnosis of acromegaly. The patient was put on antibiotics, nonsteroidal antiinflammatory drugs and isotretinoin in a dose of 1 mg/kg/day, which was increased to 1.5 mg/kg/day. Except for an initial mildly beneficial response, the skin lesions were largely resistant to high doses of isotretinoin at the end of four months. Discussion Acromegaly, the clinical state of growth hormone (GH) hypersecretion, is usually the result of somatotropic adenomas but is also caused by extrapituitary lesions in some rare cases. [5] GH stimulates synthesis of collagen and glycosaminoglycan in the skin and skeleton leading to insidious hypertrophy of skin, subcutaneous tissue and viscera and to periosteal overgrowth. GH also causes increase in size and function of sweat glands and sebaceous glands as seen in acromegaly, which results in an offensive odor and exacerbation of acne. Acne conglobata, an uncommon and severe form of acne, usually appears in early teens and becomes increasingly active in the second to third decade of life. Acute anterior uveitis, [6] renal amyloidosis [7] and IgA gammopathy [8] have been reported with AC. The primary cause of AC remains unknown. In our patient, the late age of onset and chronic unremitting course refractory to medical treatment was probably secondary to pituitary adenoma and related to abnormal GH levels. This rare variant of acne has not been reported till date with endocrinopathies. The archetypical lesion of acne conglobata is the nodule - a large, succulent, tender mass, often fusing to form odd-shaped aggregates, hence the name conglobata. The nodules may evolve into draining sinuses, which typically remain active for years with off-and-on discharges. There are burrowing and interconnecting abscesses and cysts containing foul-smelling and seropurulent material. Polyporous comedones are the most extraordinary finding. The lesions mainly involve the trunk. Healing results in disfiguring scarring, both keloidal and atrophic. The course of AC is chronic and the prognosis is poor. Squamous cell carcinoma has been reported to arise in chronic scars of AC. [9] Treatment is difficult and often ineffective. Intensive antibiotic therapy is necessary. Systemic steroids are effective but long-term therapy is necessary. The use of isotretinoin has produced prolonged remission [10] and is considered the treatment of choice. In our patient, isotretinoin was largely ineffective. This case is being reported for the unusual features of acne conglobata, i.e. , its onset in the latter part of the 4 th decade of life, localization to the gluteal region and resistance to high doses of isotretinoin and association with acromegaly. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08050f2.jpg] [dv08050f1.jpg] [dv08050f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}