 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
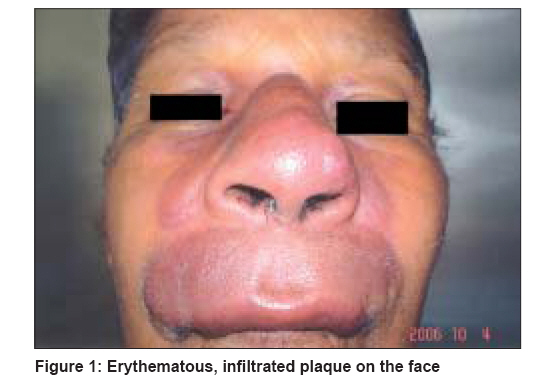
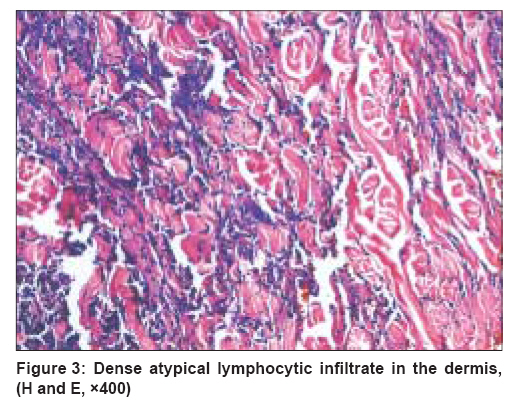
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 2, March-April, 2008, pp. 145-147 Case Report Nasal NK/T cell lymphoma presenting as a lethal midline granuloma Mehta Vandana, Balachandran C, Bhat Sudha, Geetha V, Fernandes Donald Department of Skin and STD, Kasturba Medical College, Manipal Code Number: dv08052 Abstract Nasal NK/T cell lymphomas are aggressive, locally destructive, midfacial, necrotizing lesions. The nonspecific clinical symptoms constitute a major stumbling block in the early diagnosis and management of these lymphomas. We report here a case of probable nasal NK/T cell lymphoma in an apparently healthy male that progressed rapidly in a short span of time and was managed subsequently with chemotherapy and external beam irradiation with which the lesion regressed. Keywords: Lymphoma, Midline granuloma, Nasal Introduction Lethal midline granuloma also known as ′Stewart′s granuloma′ or ′polymorphic reticulosis′ refers to the presence and sequelae of a destructive lesion in the upper respiratory tract. According to literature, the majority of lethal midline granulomas are nasal NK/T cell lymphomas. [1] Nasal NK/T cell lymphomas are aggressive, locally destructive, midfacial, necrotizing lesions. Most of them were initially diagnosed as lethal midline granuloma, a term that is slowly being phased out. The nonspecific clinical symptoms constitute a major stumbling block in the early diagnosis and management of these lymphomas. Thus, we need to be aware of the uncommon presentations of this lymphoma. We report here a case of nasal NK/T cell lymphoma in an apparently healthy male that progressed rapidly in a short span of time.Case Report A 74 year-old healthy male presented with eight month-old complaints of erythema and swelling involving the nose and upper lip. Erythema started insidiously over the inner canthus of the right eye, which slowly progressed to involve the nose, upper lip and malar area and was later associated with swelling. There was no history of nasal stuffiness; however, the patient complained of blood-stained nasal discharge. There was no history of photosensitivity, hypopigmented, hypnoanesthetic skin lesions, sensory or motor weakness or any systemic symptoms such as fever and night sweats. Cutaneous examination revealed diffuse erythema on the nose, malar area and upper lip extending up to the eyes [Figure - 1]. Phymatoid enlargement of the nose was seen with bilaterally widened nasal cavities. A single oral ulcer with mild slough was also present on the upper labial mucosa. There was no lymphadenopathy. All the routine hematological and biochemical investigations such as hemogram, urinalysis, fasting and postmeal blood sugar, liver function tests, renal function tests were normal except for a raised ESR and absolute eosinophil count. HIV-ELISA and HBs-Ag tests were negative. Nasal endoscopic smears for fungi and mycobacteria were negative. A CT scan of the osteomeatal complex and X-ray of paranasal sinuses showed only a mild haziness in the maxillary sinuses. Skin biopsy was inconclusive with only numerous proliferating capillaries dissecting the collagen bundles with a perivascular lymphoplasmacytic infiltrate. Tissue biopsy for fungal and AFB cultures was negative. Due to the increase in absolute eosinophil counts and ESR, the patient was discharged after being prescribed a three-week course of antibiotics and diethylcarbamazine. One month later, the patient presented with a sudden onset of a nodular, erythematous, vascular lesion completely occluding the left nostril with edema and erythema of the right upper lip [Figure - 2]. A repeat biopsy at this stage showed a mixed cellular infiltrate of eosinophils, lymphocytes, plasma cells and histiocytes. A diffuse dense infiltrate of atypical small and large lymphocytes with pleomorphism was present in the dermis [Figure - 3] and subcutis extending between the collagen bundles in rows, columns and cords. The abnormal cells were also seen infiltrating the skeletal muscle. Immunohistochemistry (IHC) was positive for T cell markers, i.e. , CD3 and CD45RO but was negative for a B cell marker, i.e. , CD20. IHC for an NK cell marker, i.e. , CD56 was unavailable; in spite of this, the biological behaviour of NK-positive and T-positive nasal extranodal lymphomas is similar and hence, collectively termed as NK/T cell lymphomas. Thus, based on the clinical picture and histopathology, we came to a presumptive diagnosis of extranodal nasal NK/T cell lymphoma as the IHC for an NK cell marker (CD56) was not performed. Accordingly, our patient was referred to oncology for the initiation of field radiotherapy and chemotherapy where he was given injection methotrexate 50 mg I.V. for 12 weeks along with external beam irradiation (total 34 Gy units). During his three months′ stay in the hospital. there was considerable improvement in the nasal and facial lesions. Discussion Mature or peripheral NK/T cell lymphomas account for only 10-15% of non-Hodgkin′s lymphomas. Amongst them, the most common and well-characterized ones are the ′nasal′ and ′nasal type′ NK/T cell lymphomas. They are currently referred to as angiocentric lymphomas in the Revised European American Lymphoma (REAL) classification or as nasal NK/T cell lymphoma by the World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) classification. [2] Their characteristic histological feature is an angiocentric/angiodestructive growth pattern with zonal necrosis. Both nasal and nasal type NK/T cell lymphomas reflect specific characteristics of NK cells. [3] NK cells are cytolytic cells which are active against tumor cells and cells infected with bacteria and viruses without prior sensitization. They develop in the bone marrow from a bipotential progenitor capable of differentiation into T and NK cells. Phenotypically, NK cells appear commonly as small lymphocytes with azurophilic granules and immunophenotypically, they express the characteristic marker CD56. Due to a common ontogeny with T cells, NK cells also express some T cell markers. Nasal NK/T cell lymphomas have a predilection for the nasal cavity and the upper aerodigestive tract although the skin and soft tissues may be involved. They are rare and are mainly seen in Asia and Latin America. Elderly males in the age group of fifty years and above are affected. The most common presentation is a chronic nasal obstruction or a purulent rhinorrhea. [4] Systemic symptoms such as fever and weight loss are absent or are observed only in advanced cases. The skin is the most common site of involvement after the nasal cavity or the nasopharynx and skin involvement may be a primary or secondary manifestation of the disease. Approximately 10-20% of the nasal lymphomas have skin involvement. [5],[6] ′Nasal type′ lymphomas show the same histological features as nasal NK/T cell lymphomas but arise from extranasal sites such as the skin, gastrointestinal tract, testis, kidney, eyes and the orbit. They occur more commonly in females. Epstein Barr virus RNA is present in 80-100% of nasal NK/T cell lymphoma cases and less often (15-40%) in nasal type NK/Tcell lymphoma cases. [7] Our patient also presented with a long history of erythematous skin lesions and blood-stained nasal discharge. IHC in this case confirmed a probable NK/T cell lineage of the tumor by demonstrating presence of CD3 and CD45RO markers and the absence of CD20 marker. Zhong et al. reported that most upper aerodigestive tract NK/T cell lymphomas were genotypically of NK cell origin and only a few belonged to T cell lineage. [7] Nasal NK/T cell lymphoma follows an aggressive and rapid downhill course in Asians with death occurring due to relapse or systemic spread in 50% of the cases. [8] Multidrug chemotherapy followed by involved field radiotherapy appears to be the most effective treatment approach. References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08052f1.jpg] [dv08052f2.jpg] [dv08052f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}